Research-Led, Evidence-Backed, Validated at Every Stage
Starting With 275 People, Not Assumptions
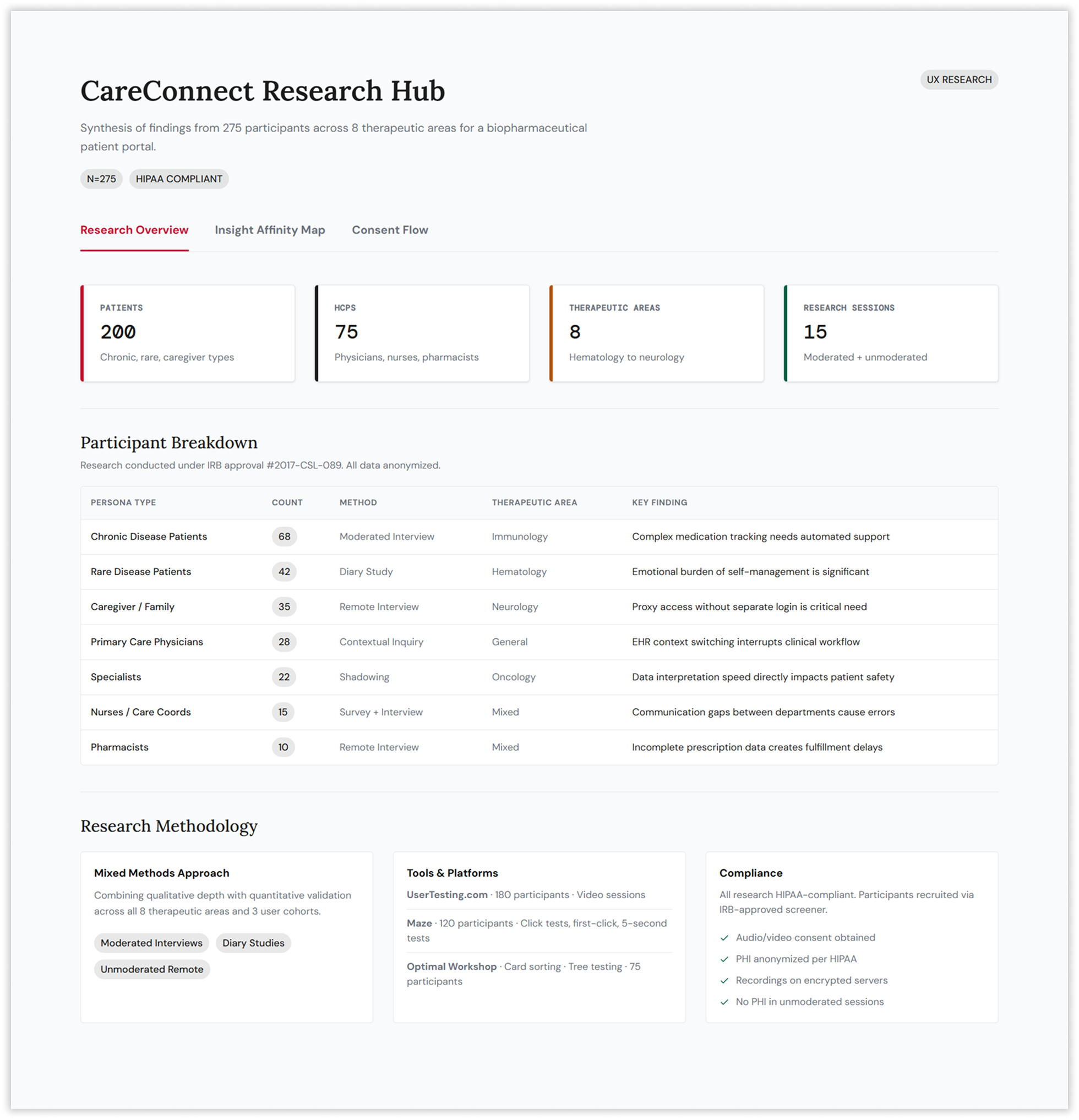
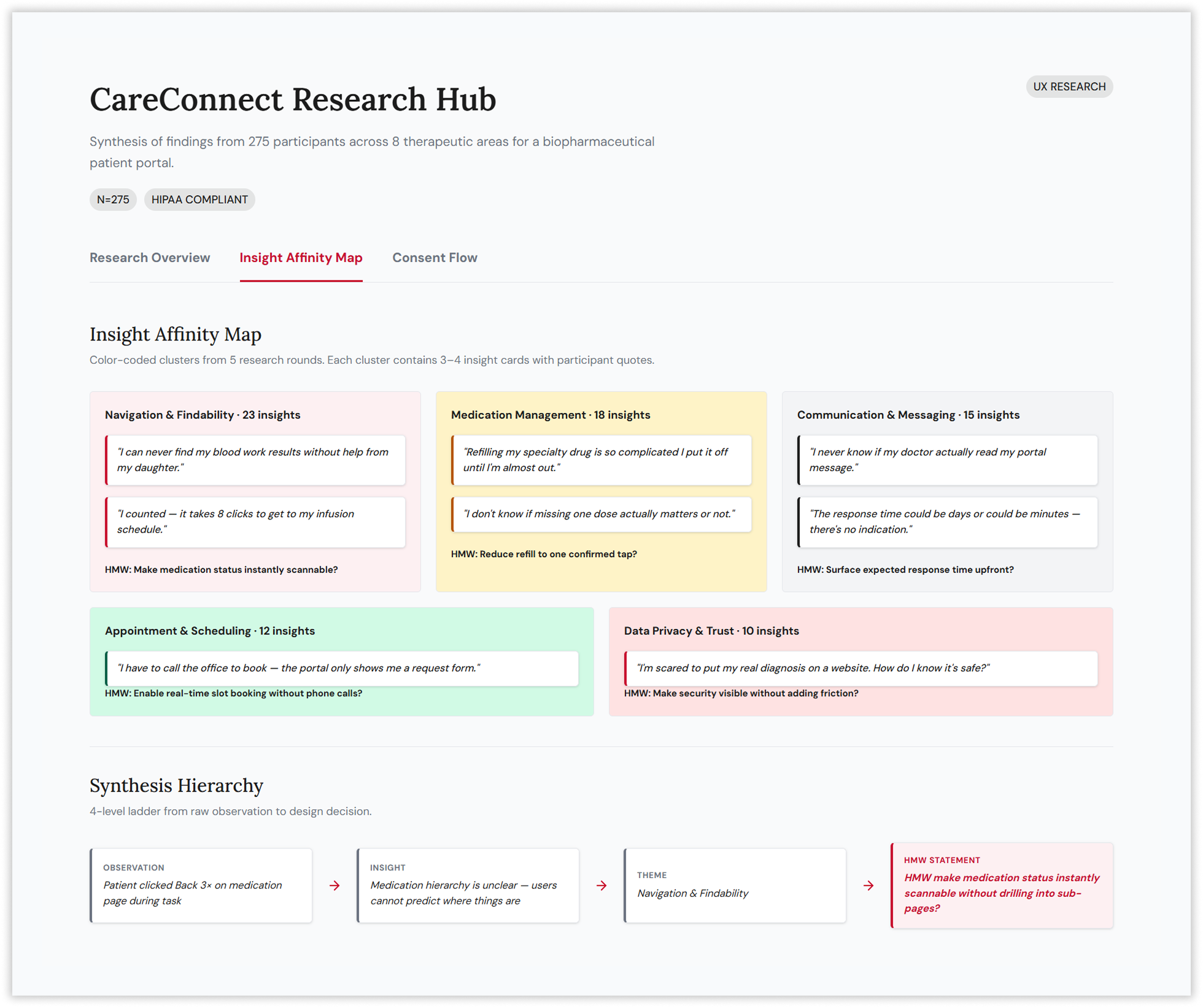
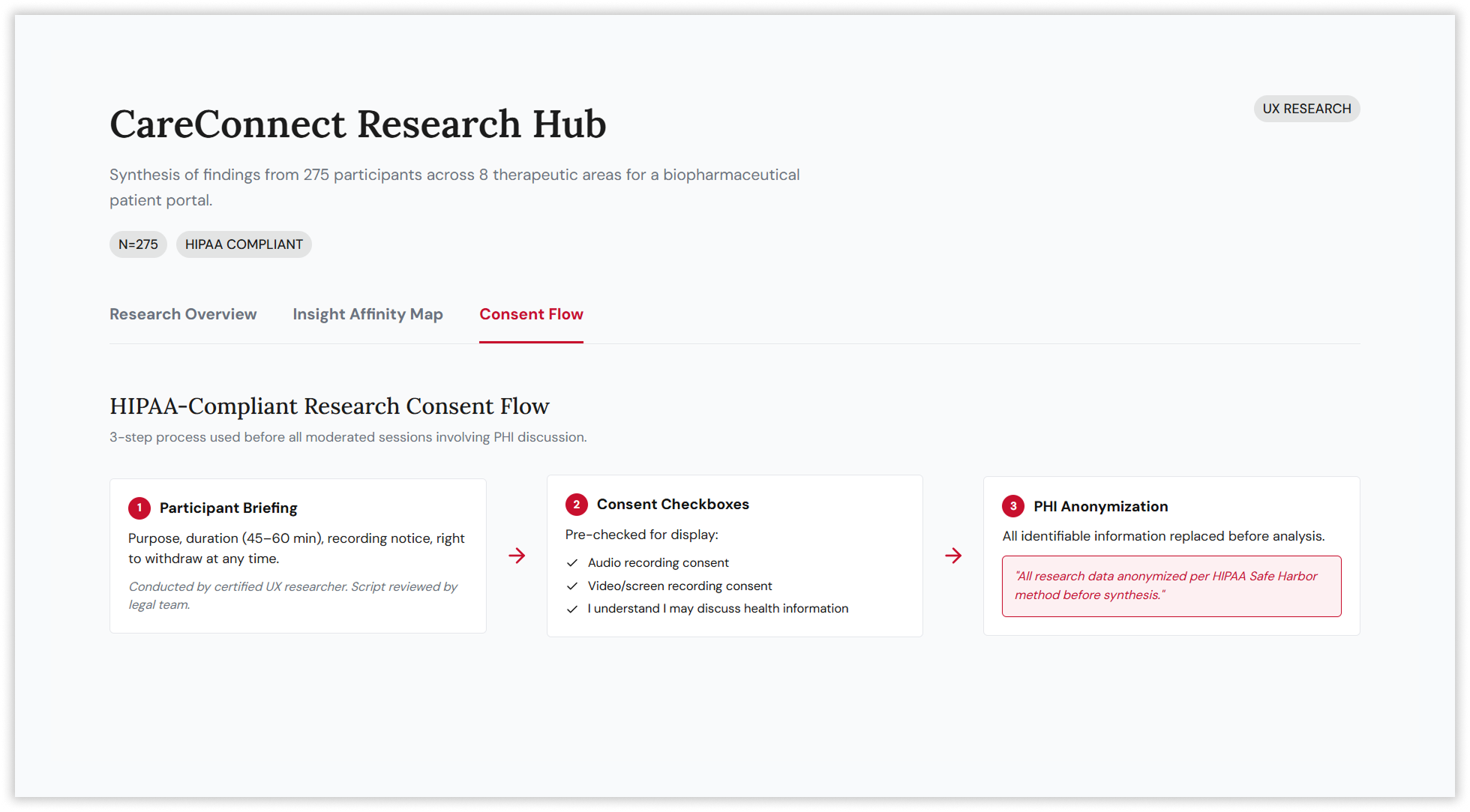
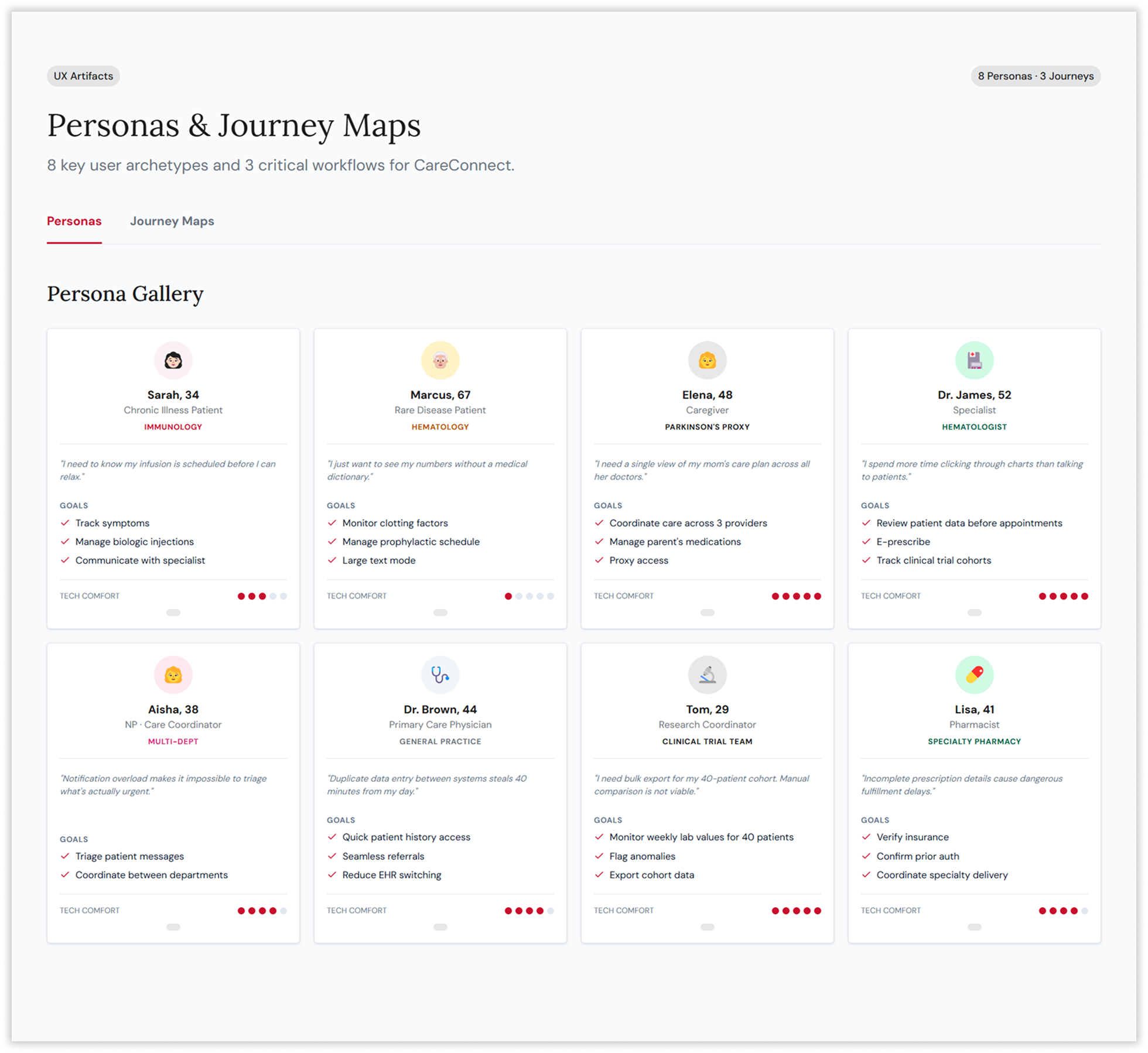
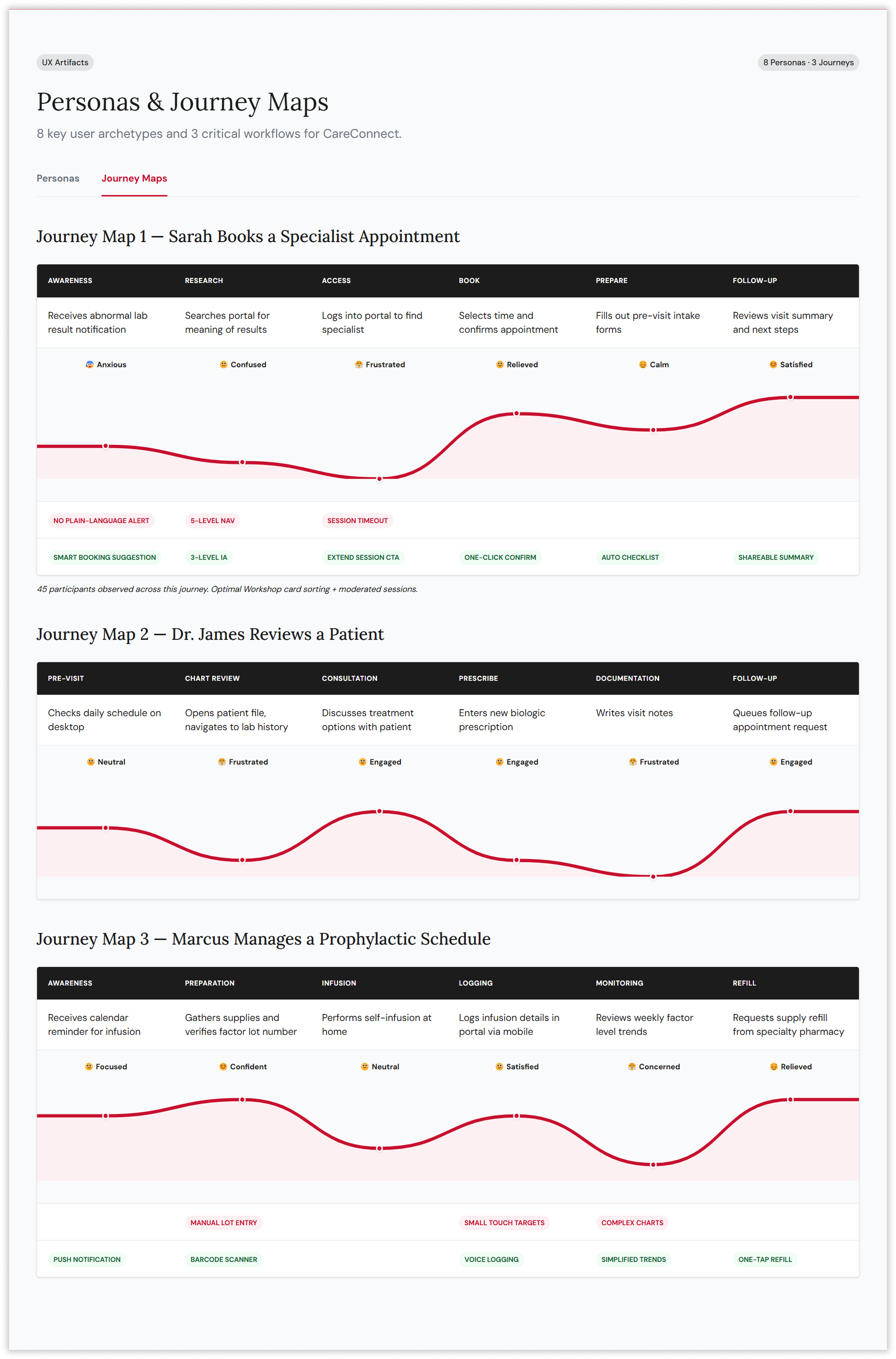
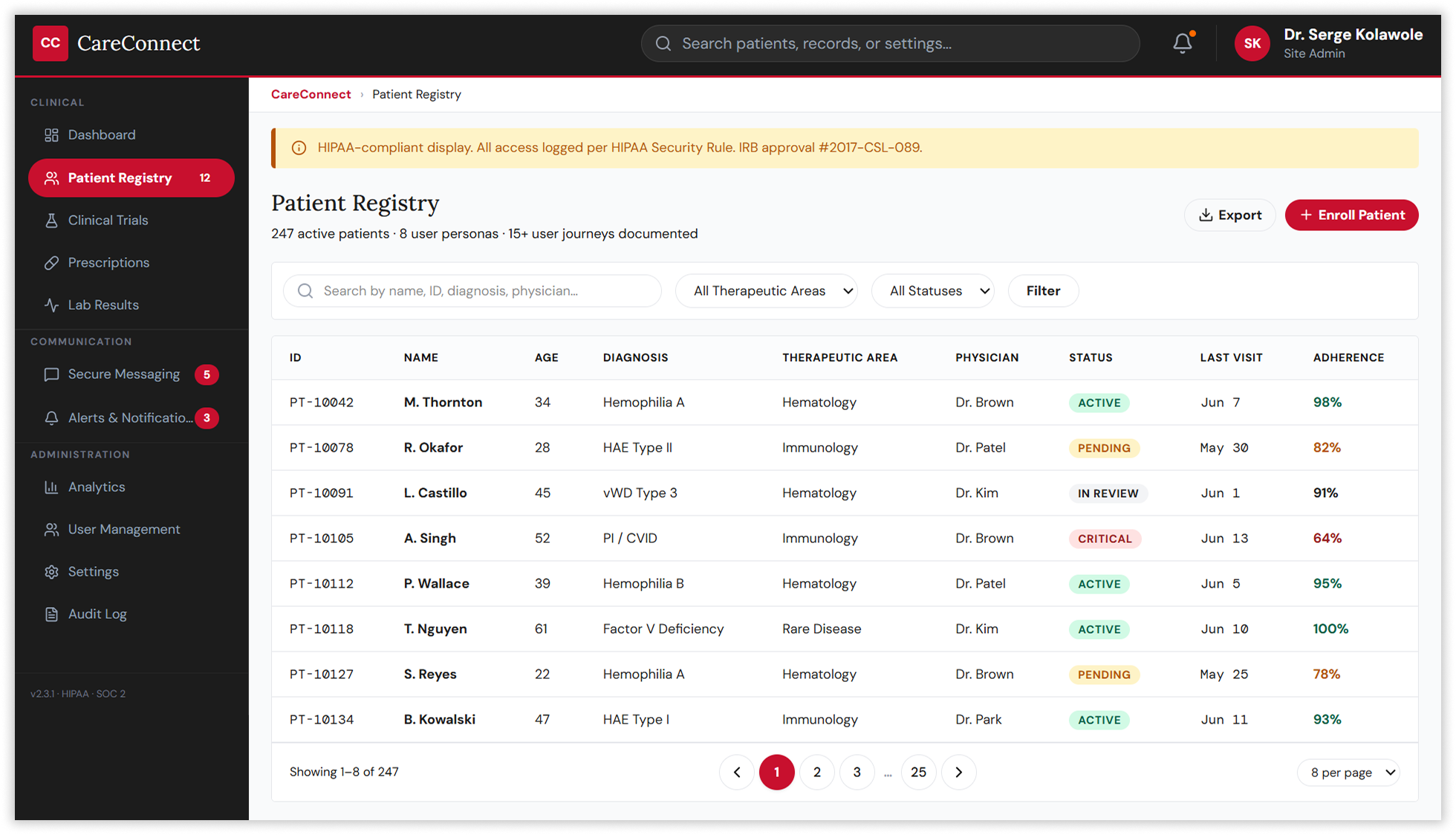
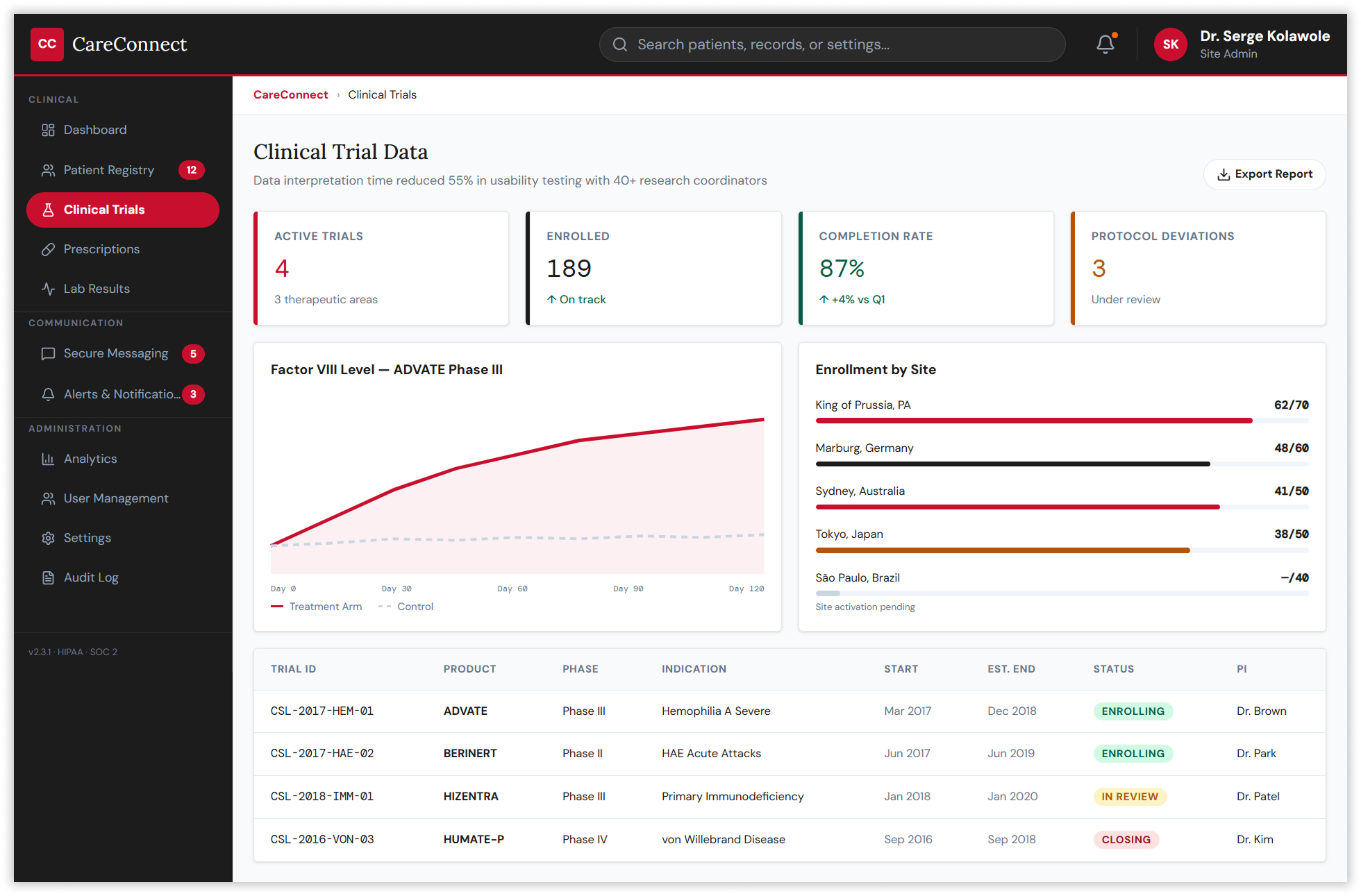
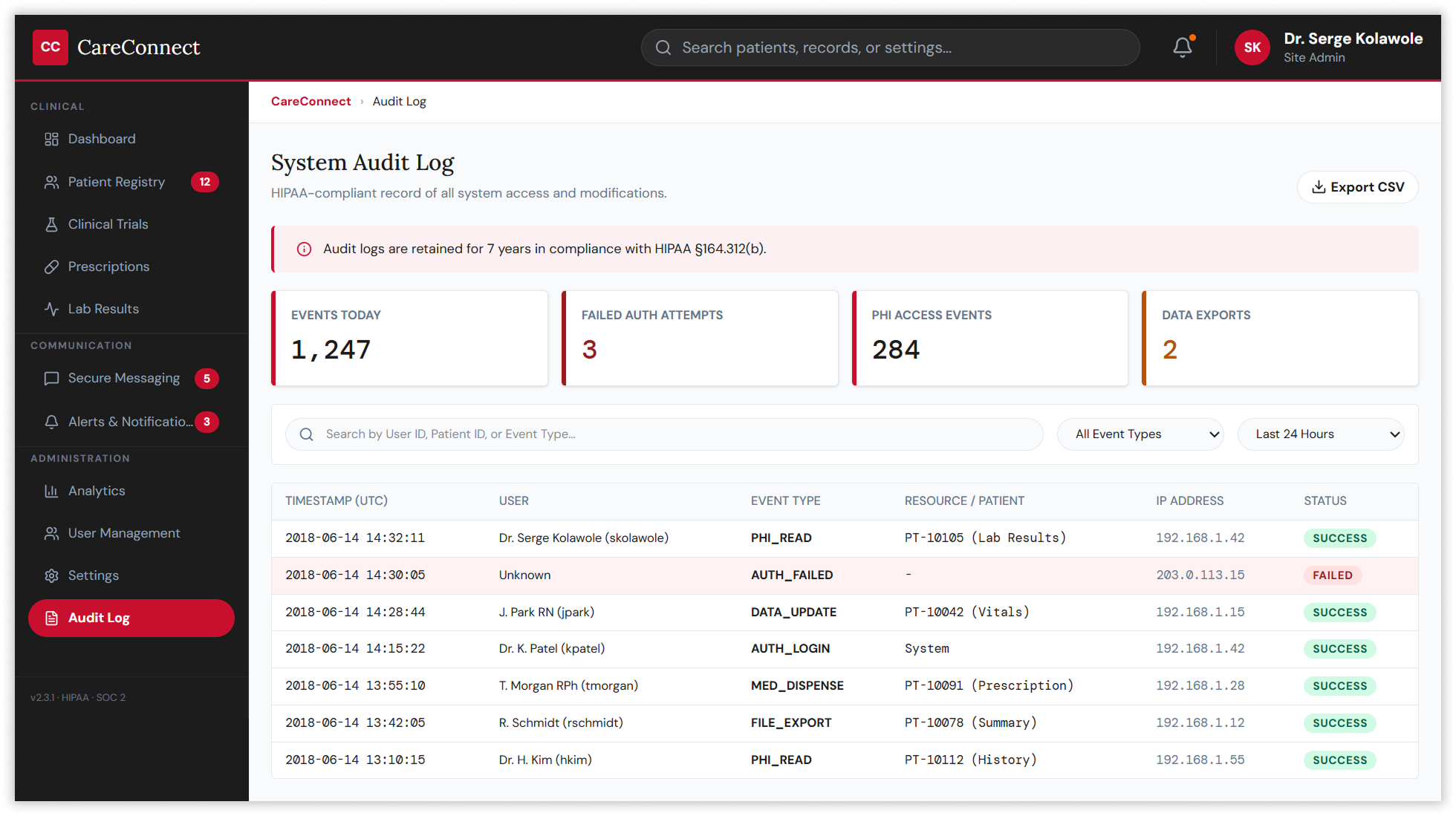
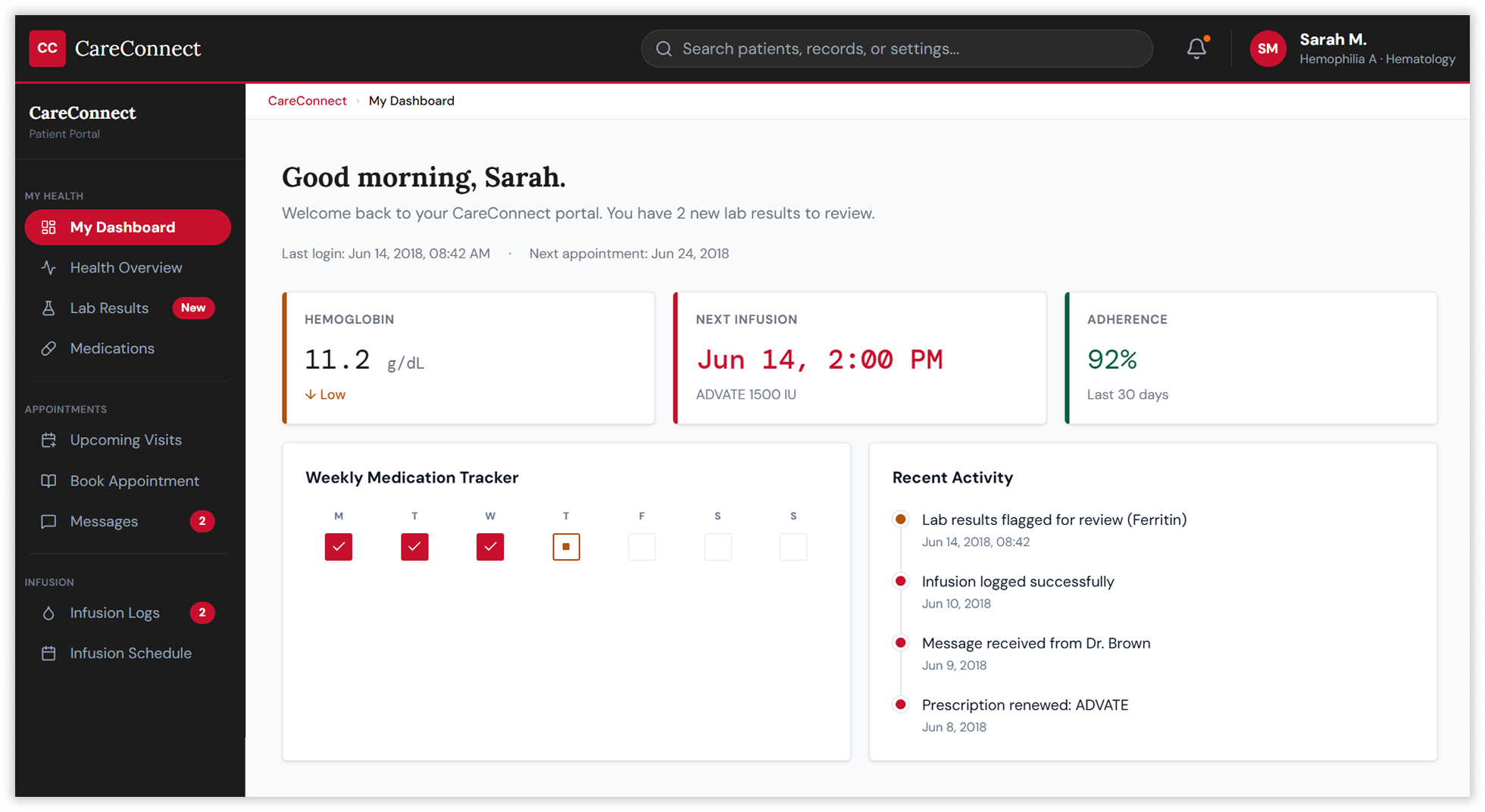
The strategy began with a comprehensive research programme spanning 200 patients and 75 healthcare professionals across eight therapeutic areas. Conducted under IRB approval and HIPAA Safe Harbor compliance, the research combined moderated interviews, diary studies, contextual inquiry, and remote unmoderated sessions to map the full landscape of user needs. Participants included chronic disease patients, rare disease patients, caregivers managing proxy access, primary care physicians frustrated by duplicate data entry, specialists demanding faster clinical data access, and research coordinators needing bulk export tools for 40-patient trial cohorts.
Making the Invisible Architecture Visible
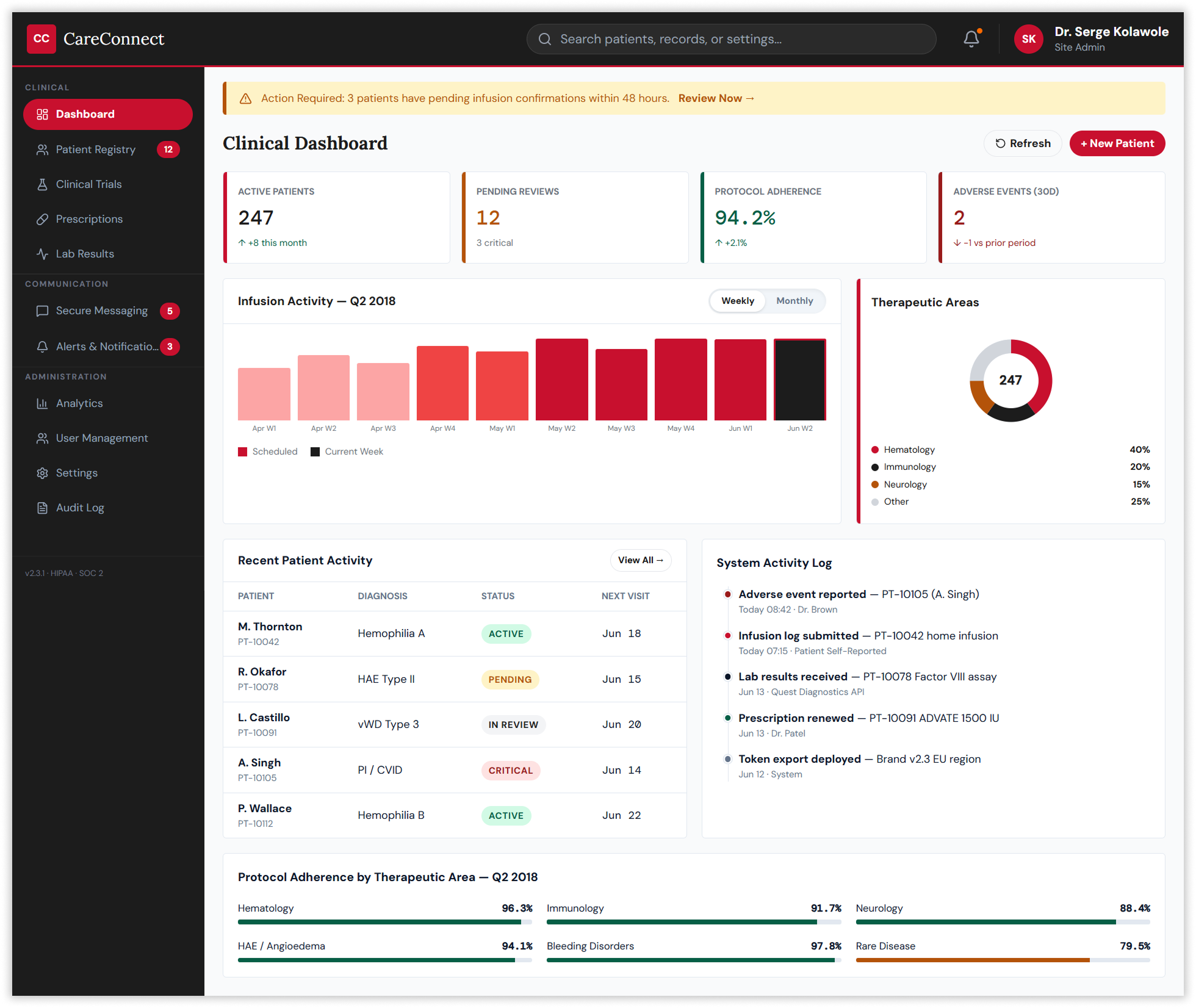
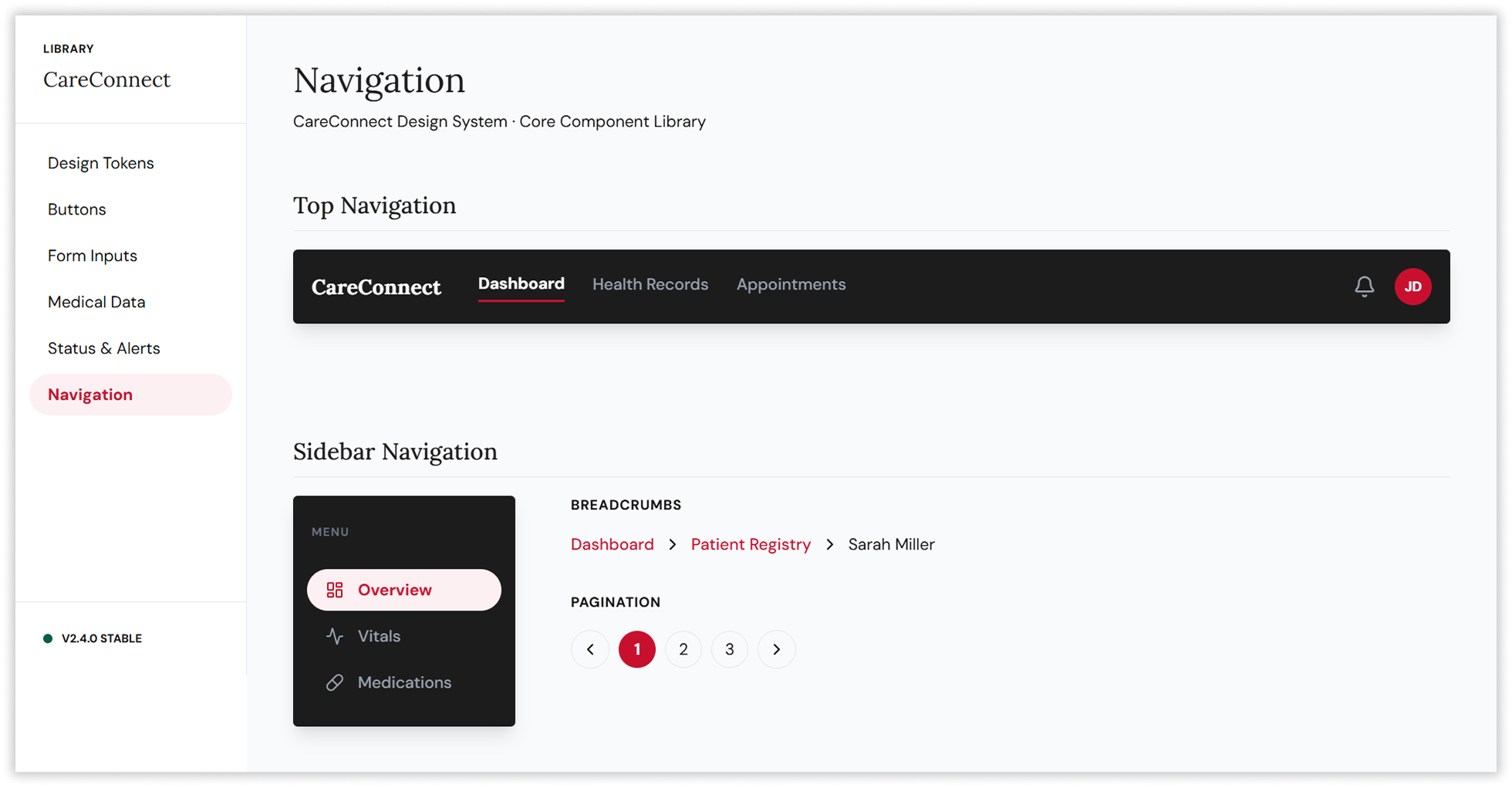
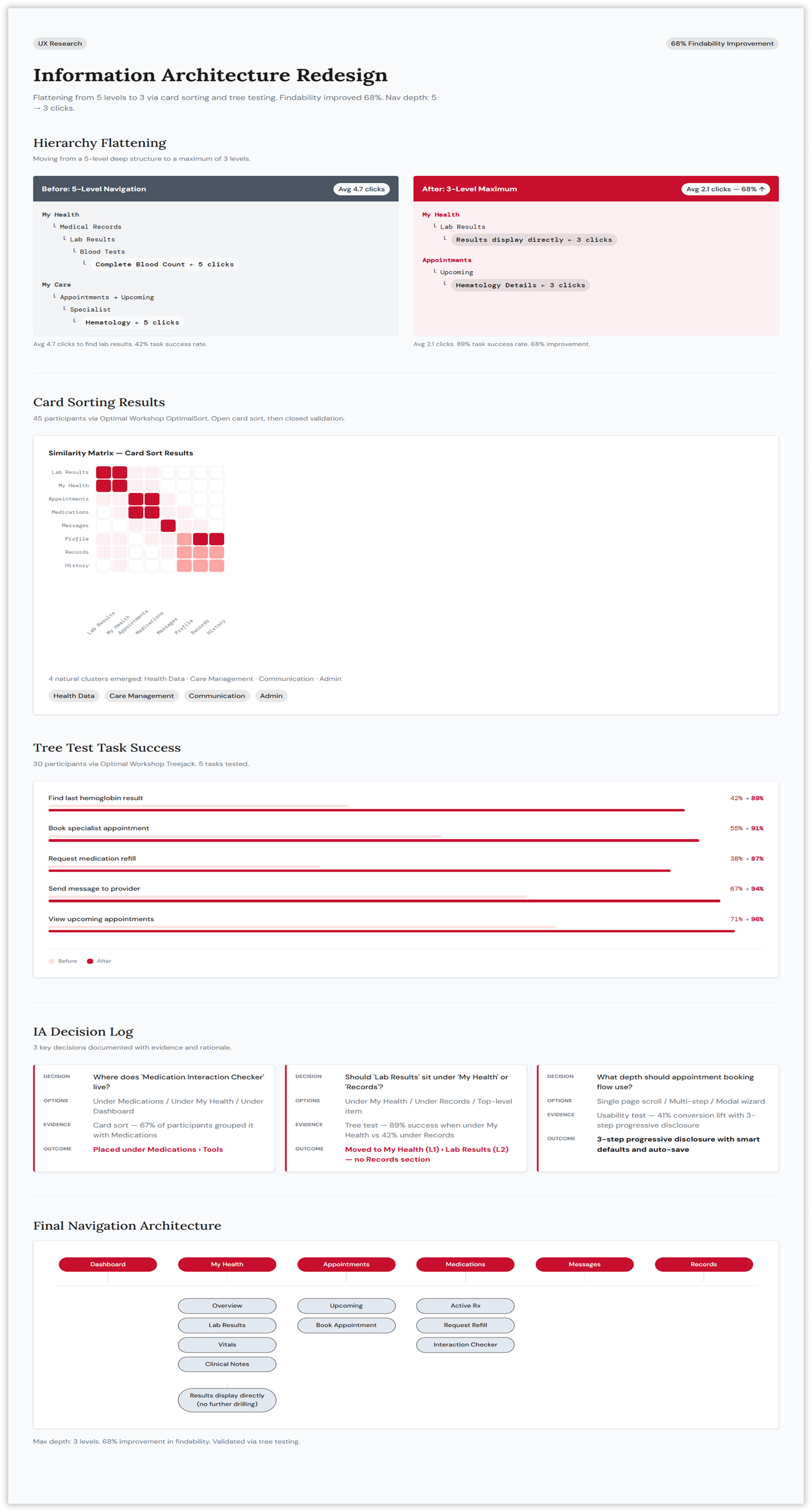
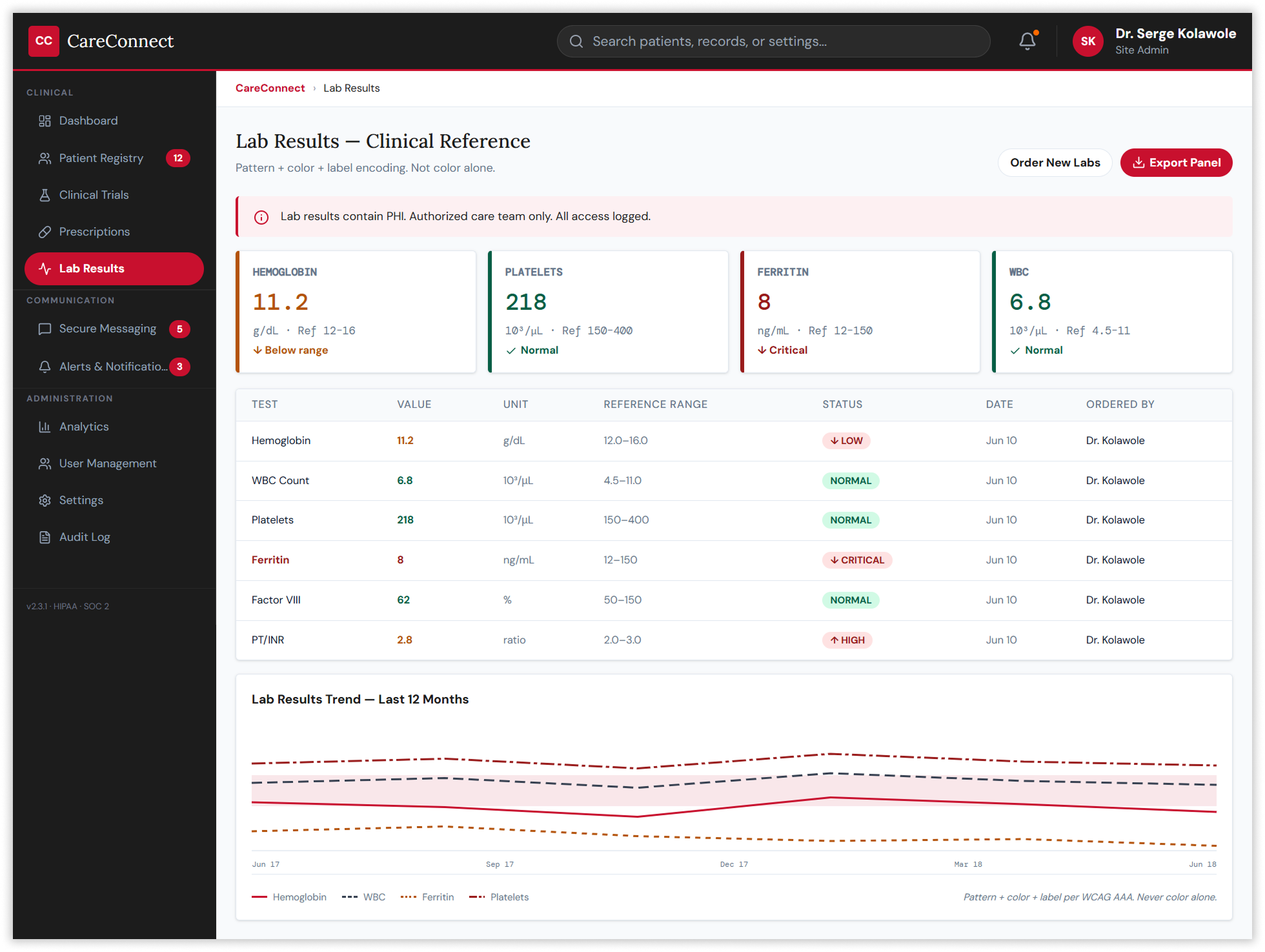
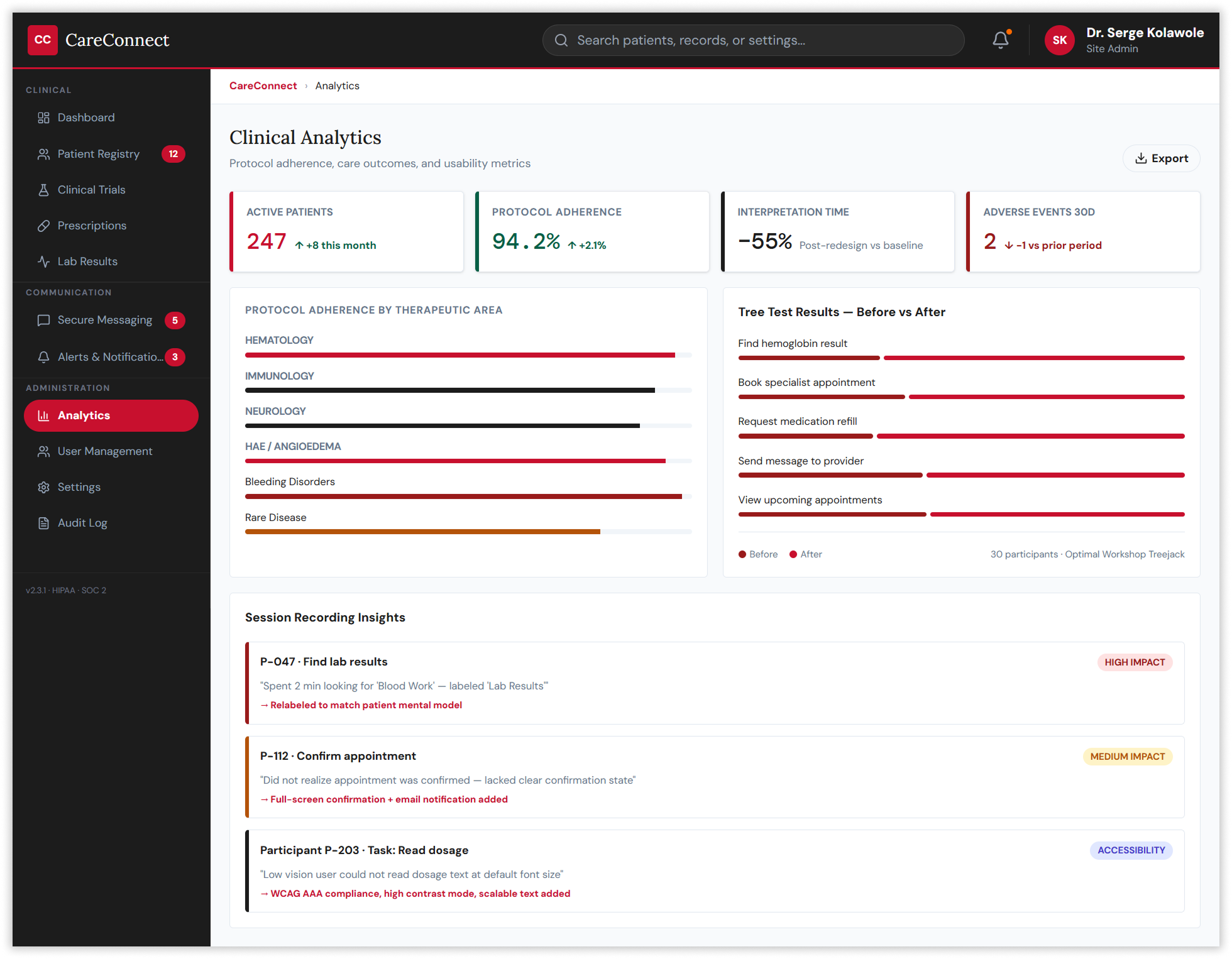
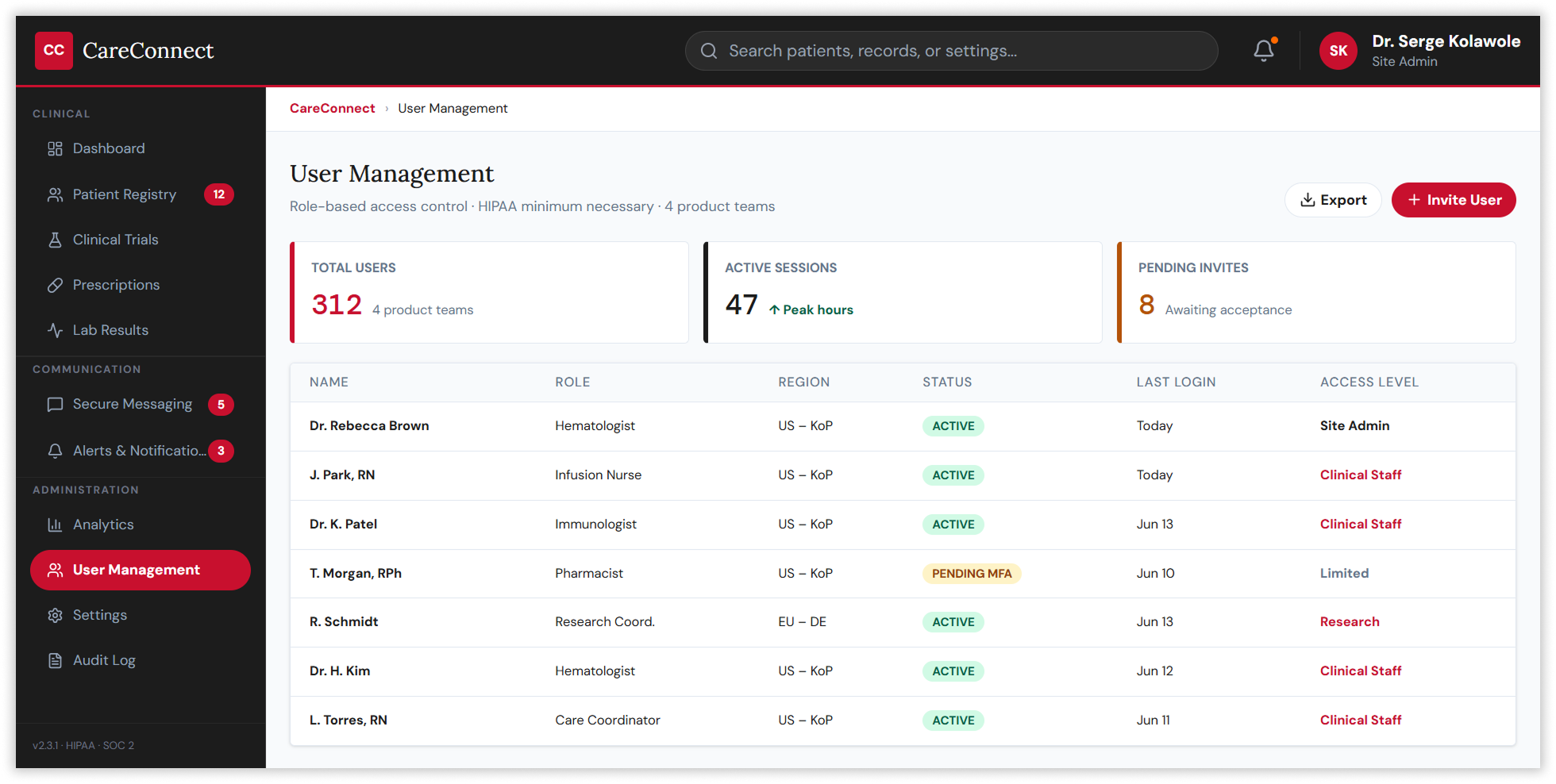
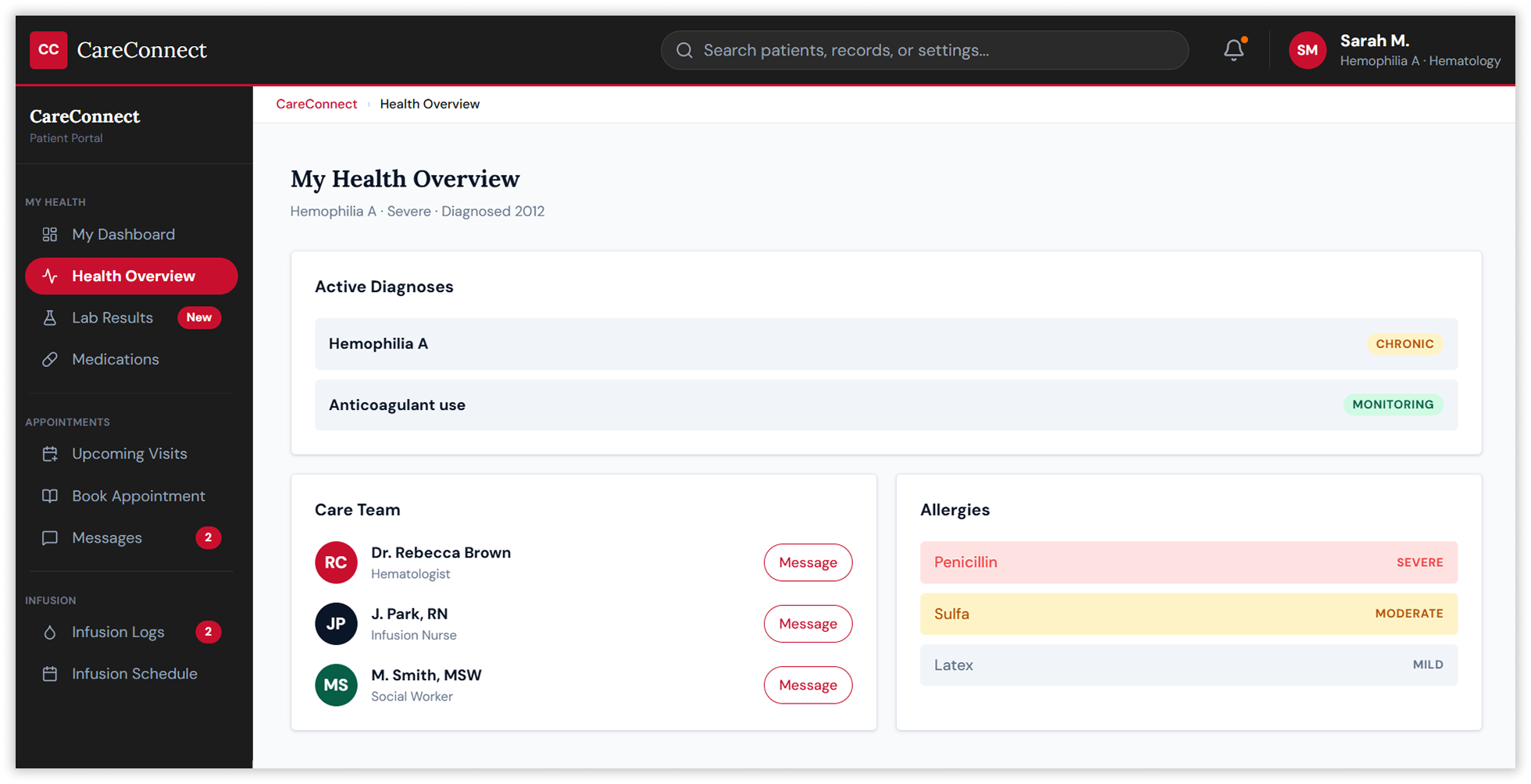
Card sorting and tree testing via Optimal Workshop with 75 participants revealed four natural information clusters — Health Data, Care Management, Communication, and Administration — that became the structural backbone of the redesigned navigation. The old five-level hierarchy was collapsed to a maximum of three, guided entirely by evidence from where users actually looked for things rather than how the system had historically organised them.
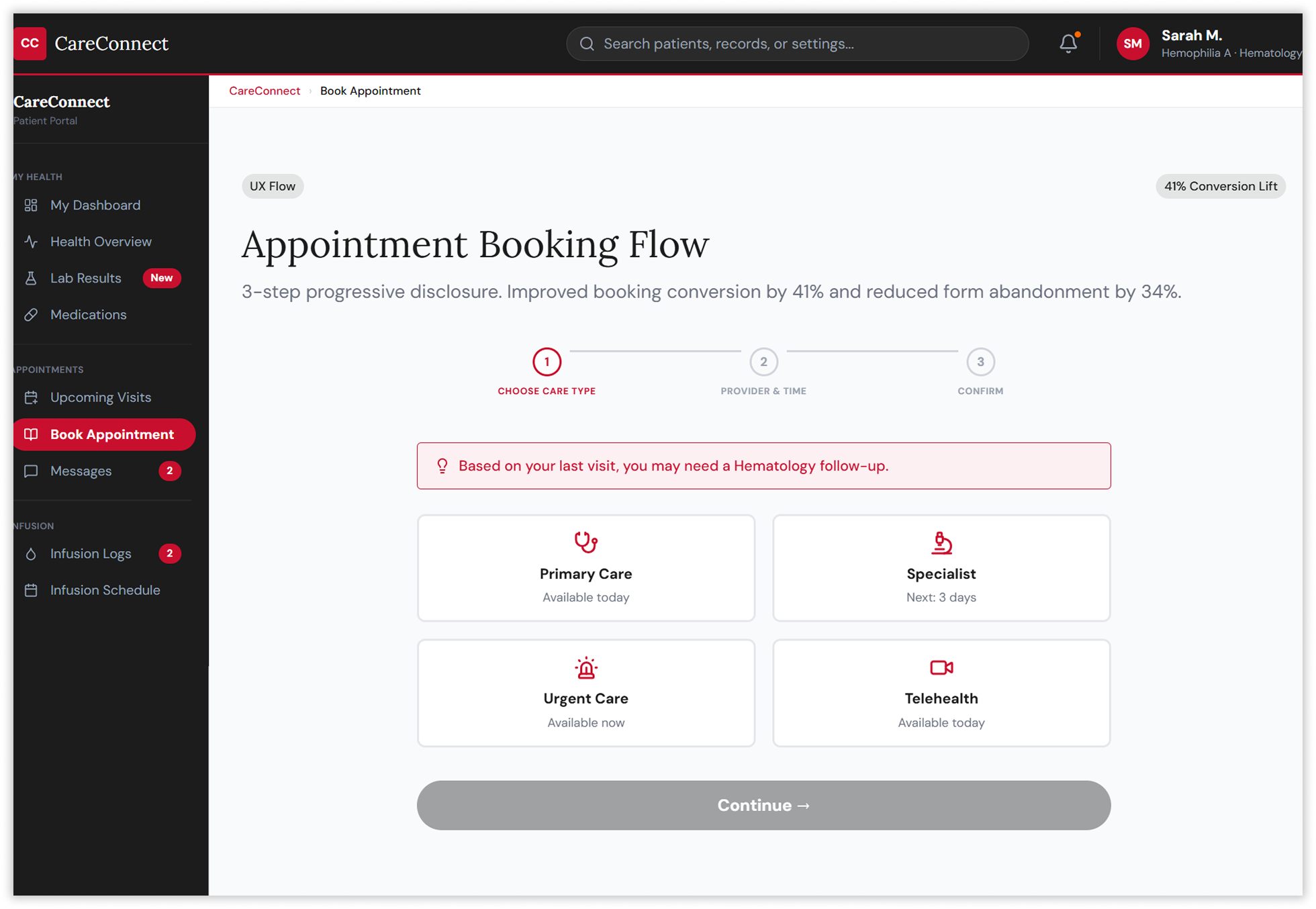
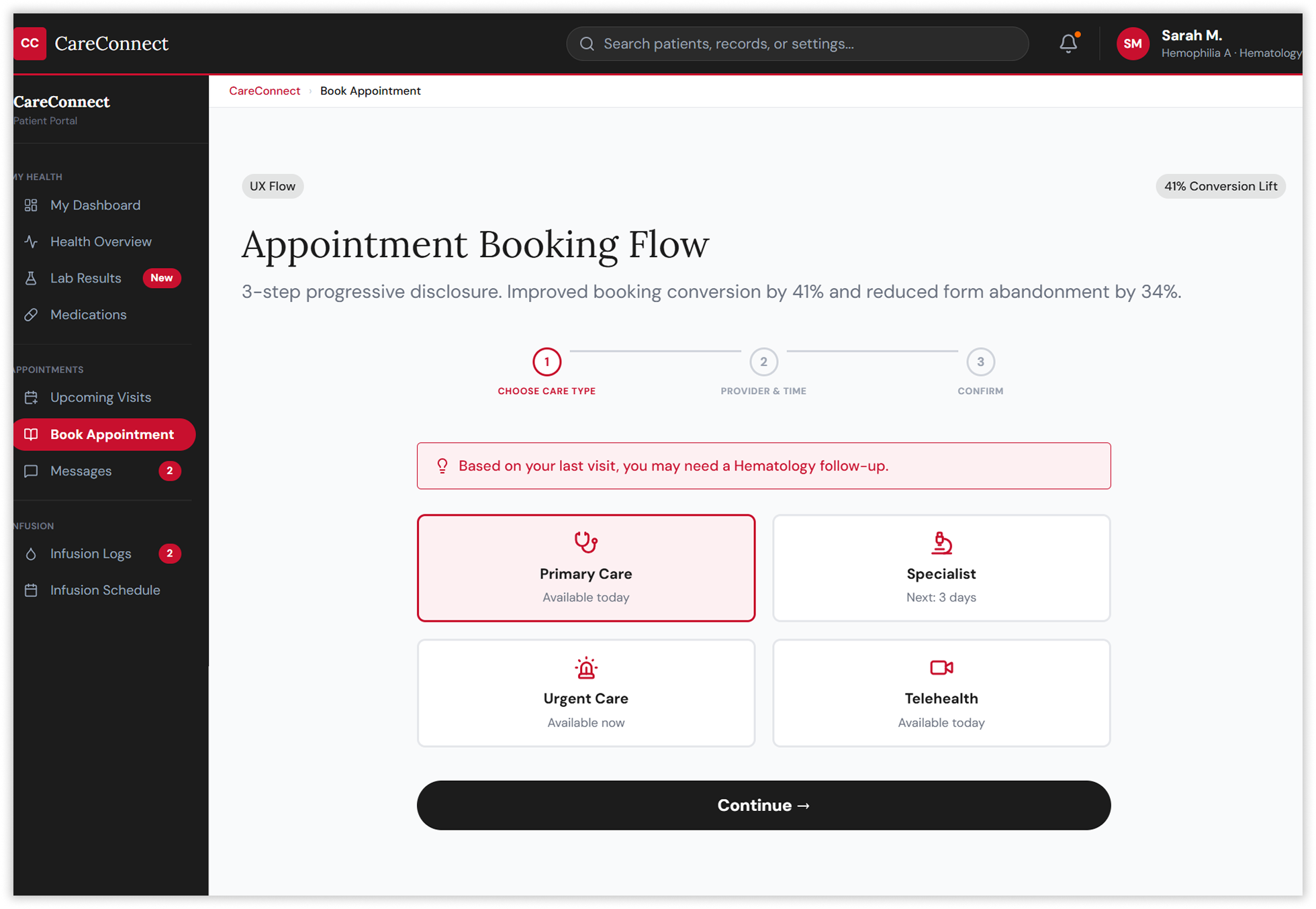
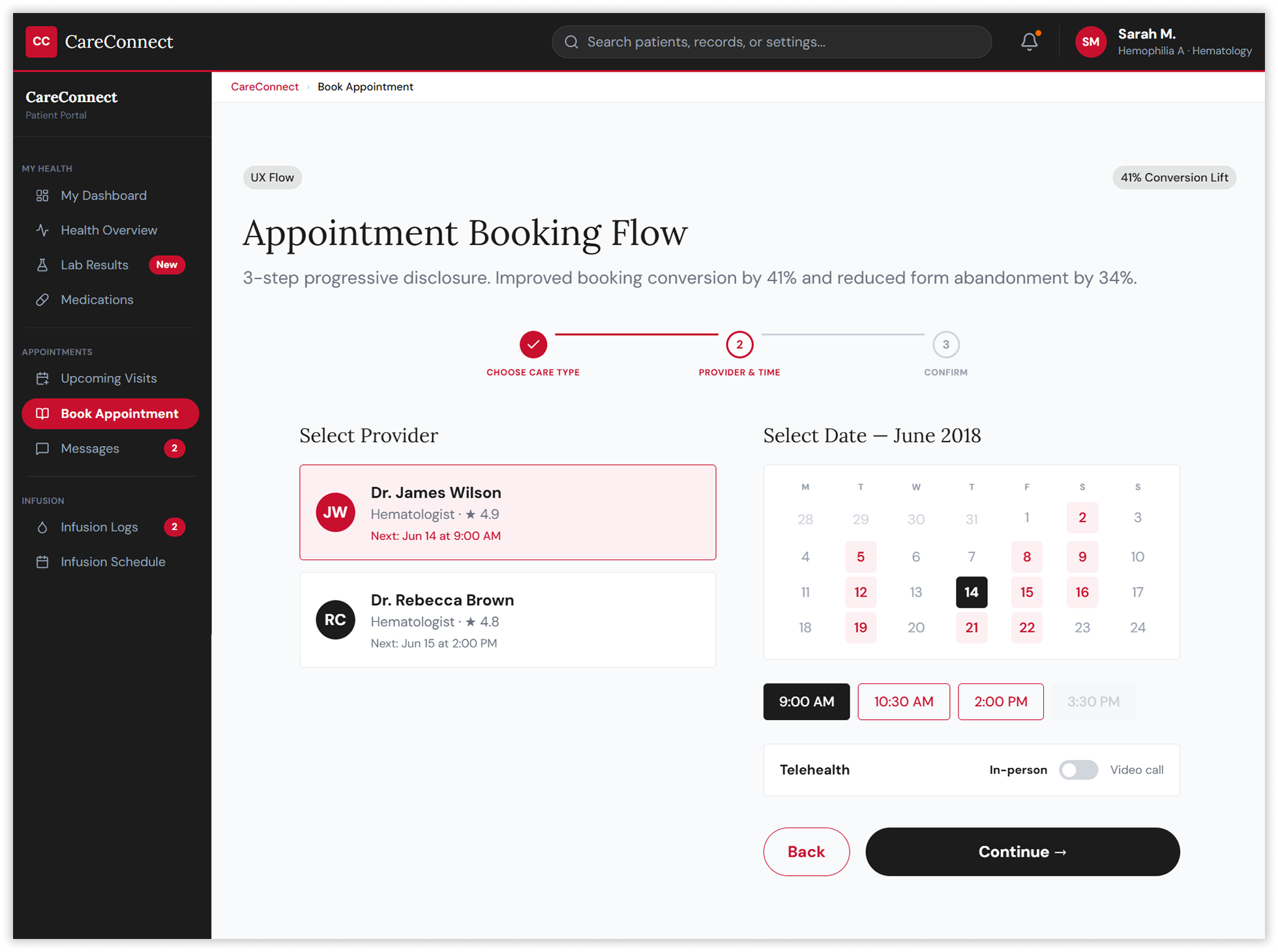
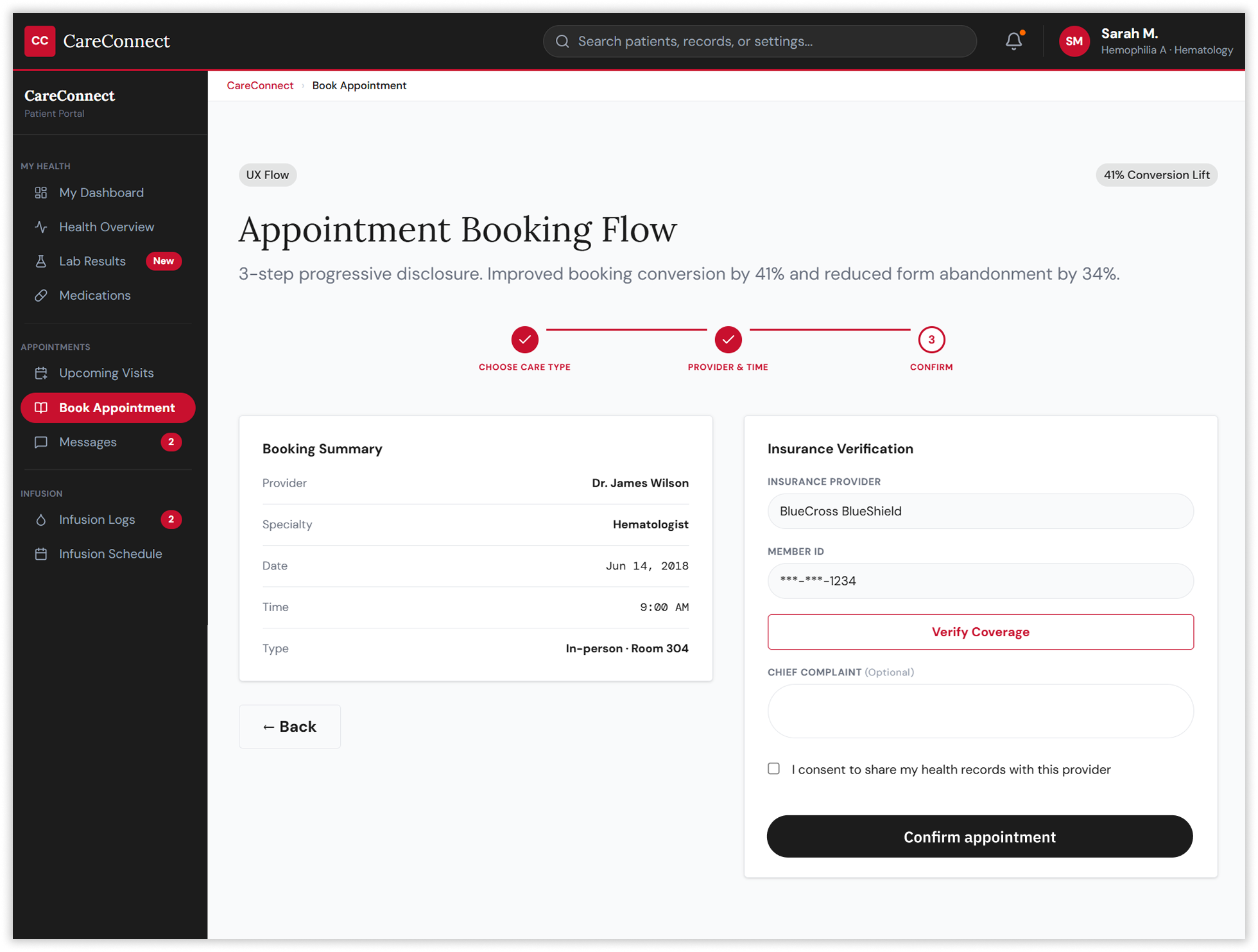
Designing Systems, Not Screens
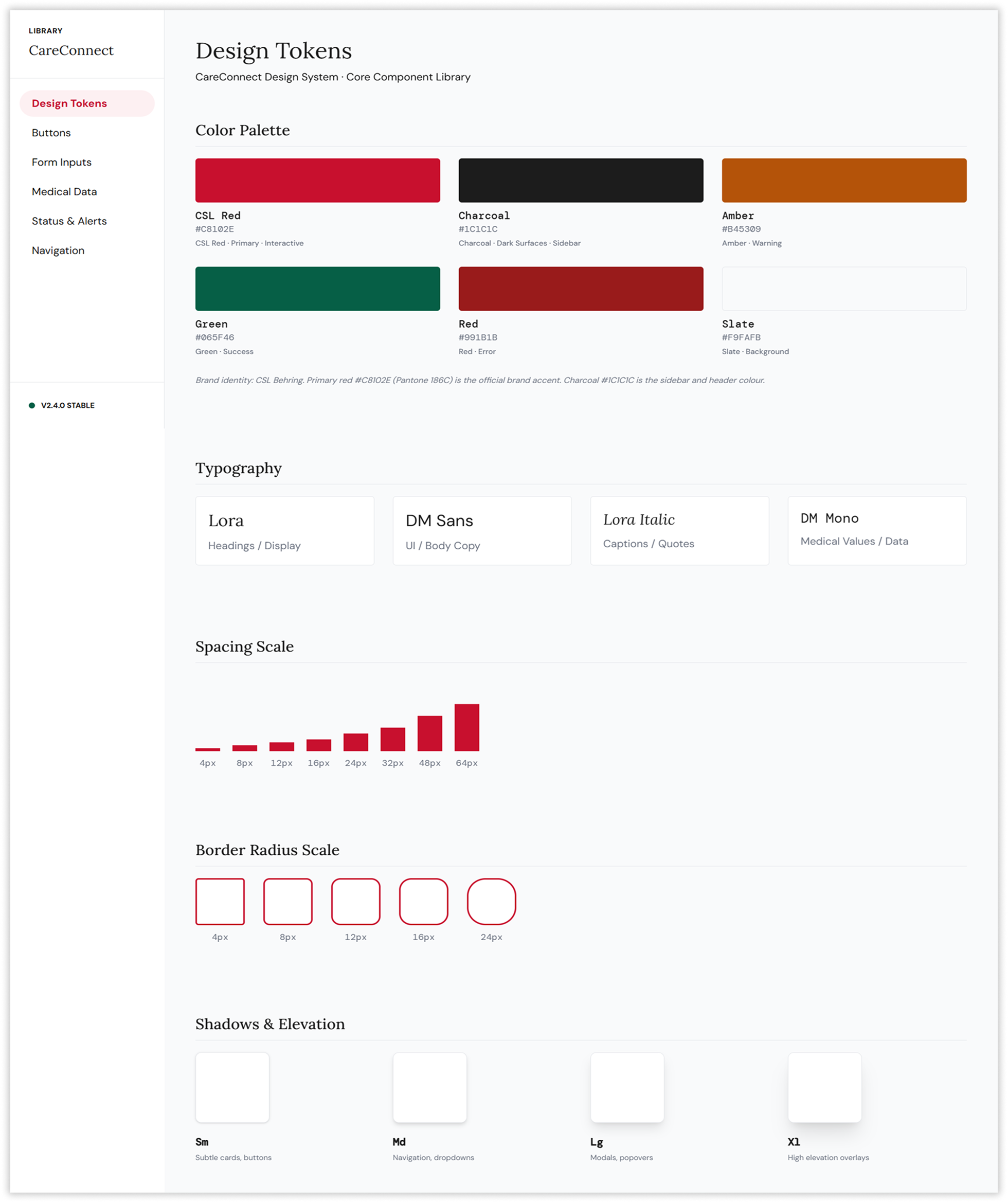
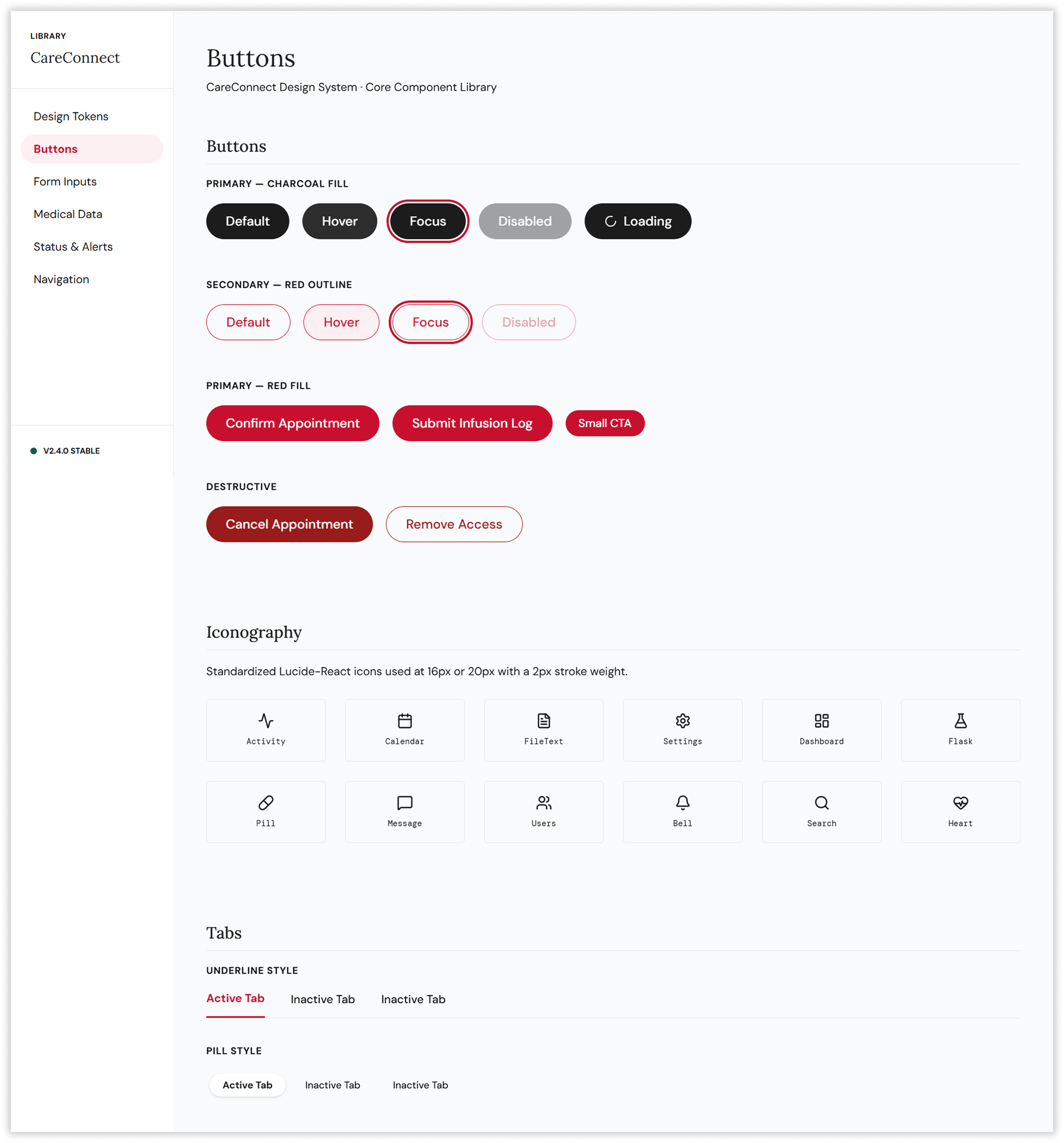
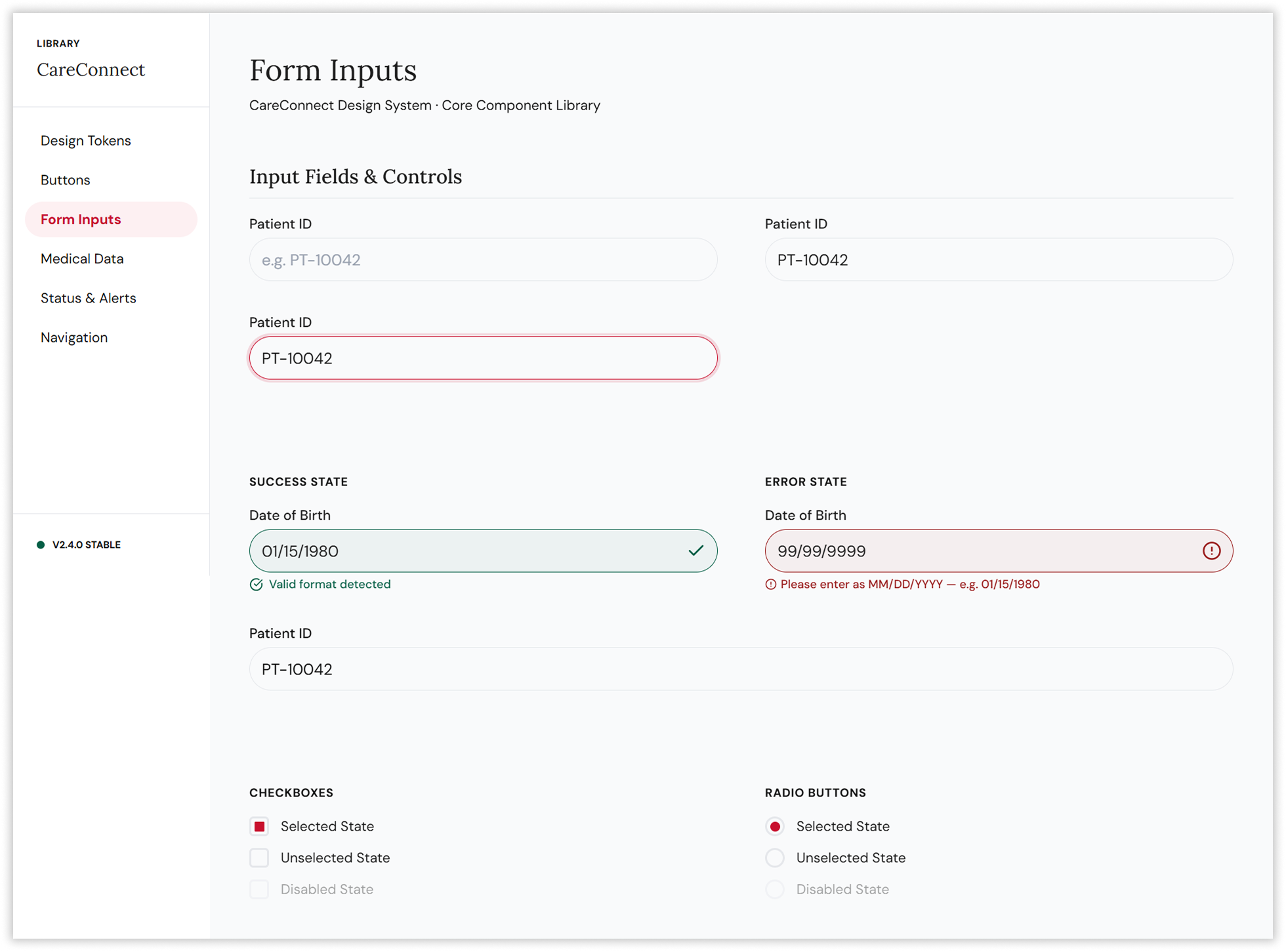
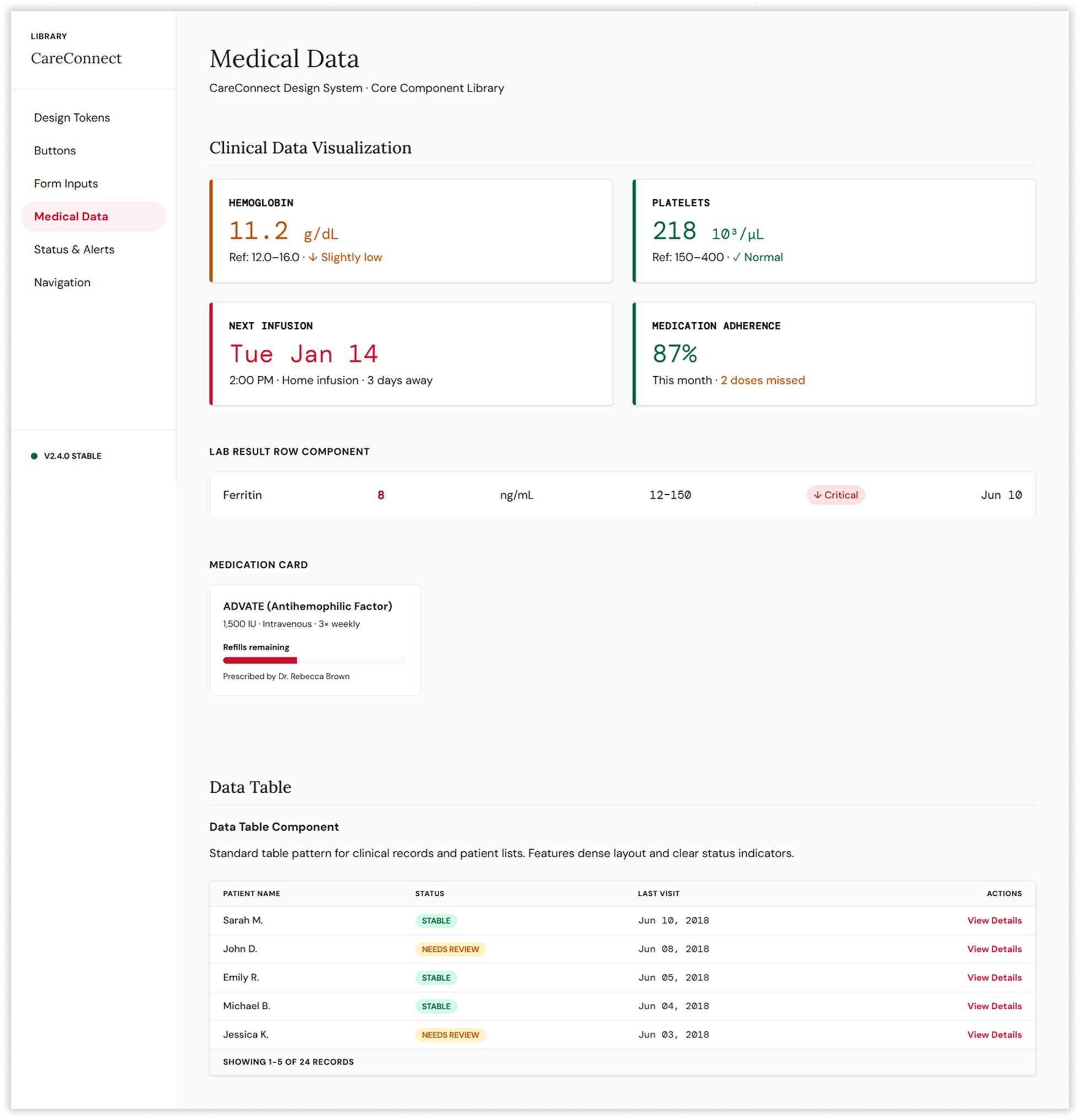
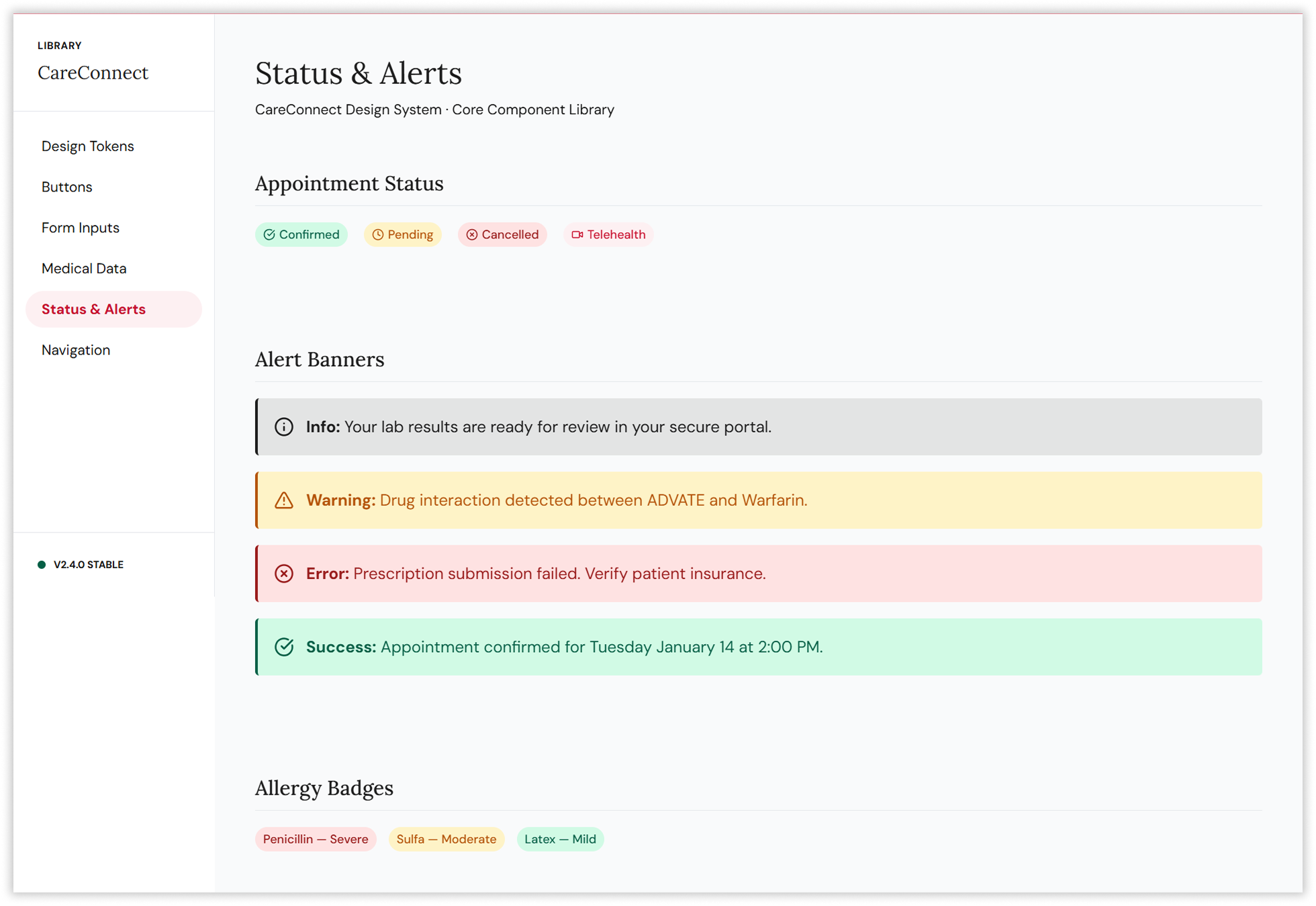
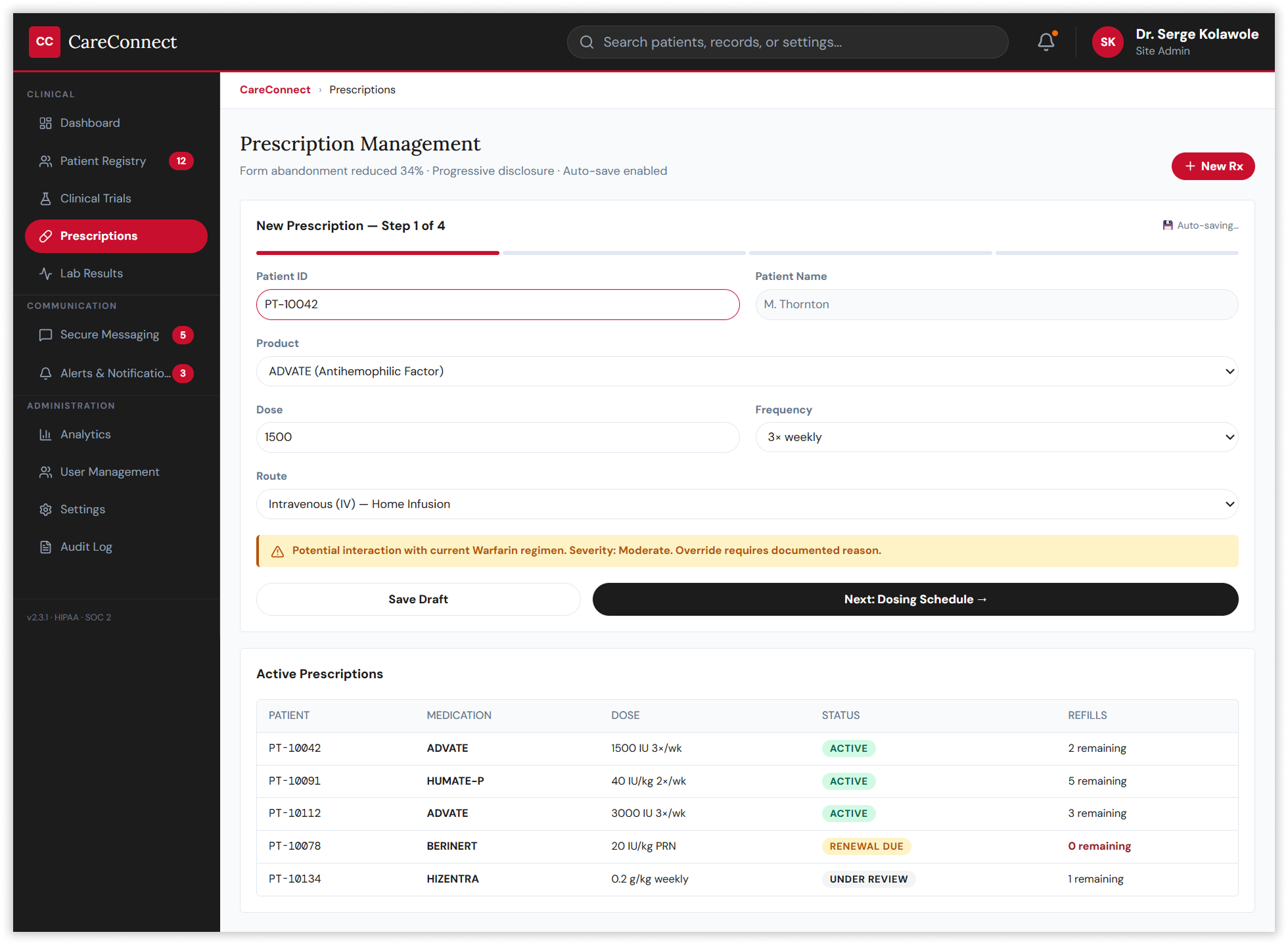
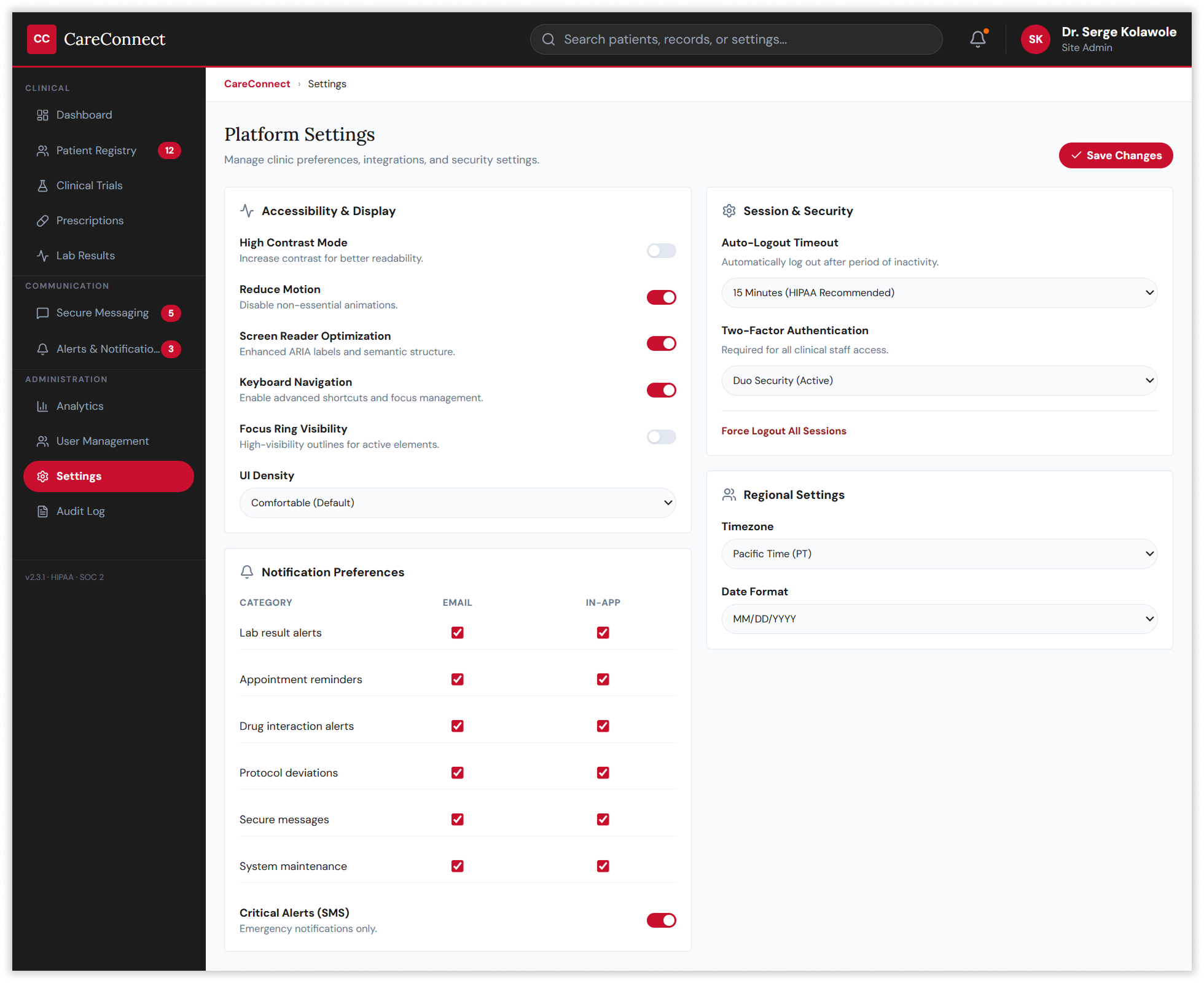
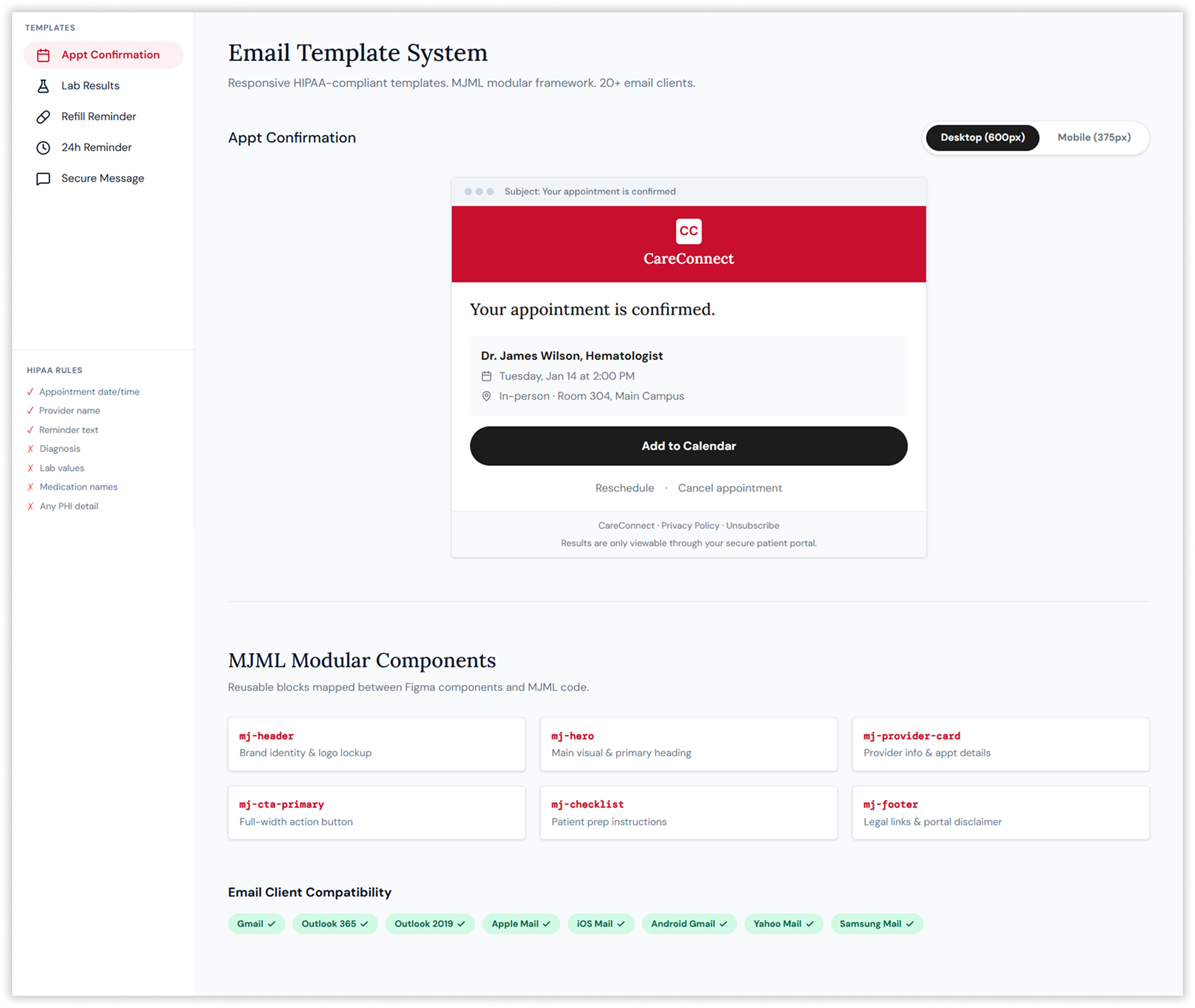
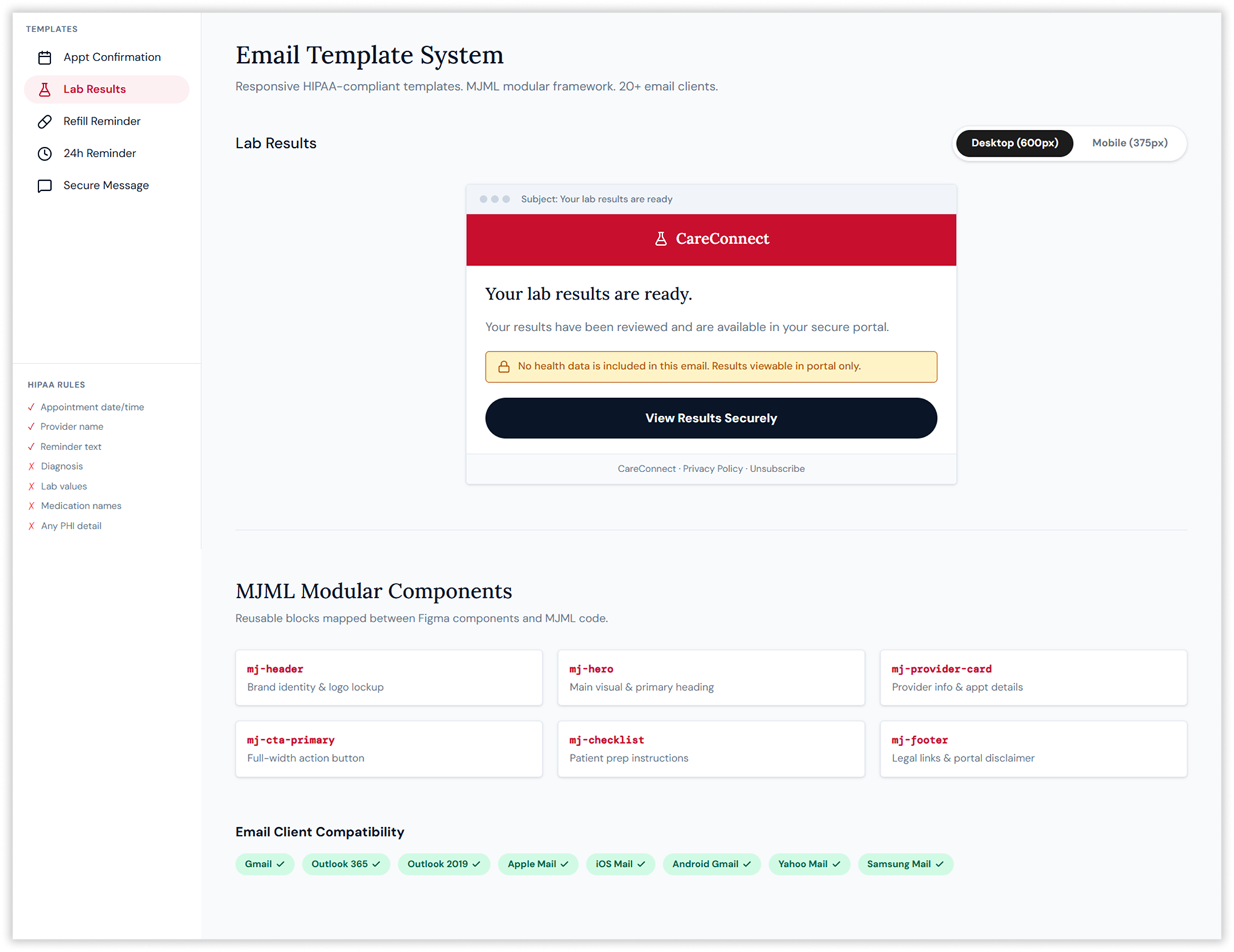
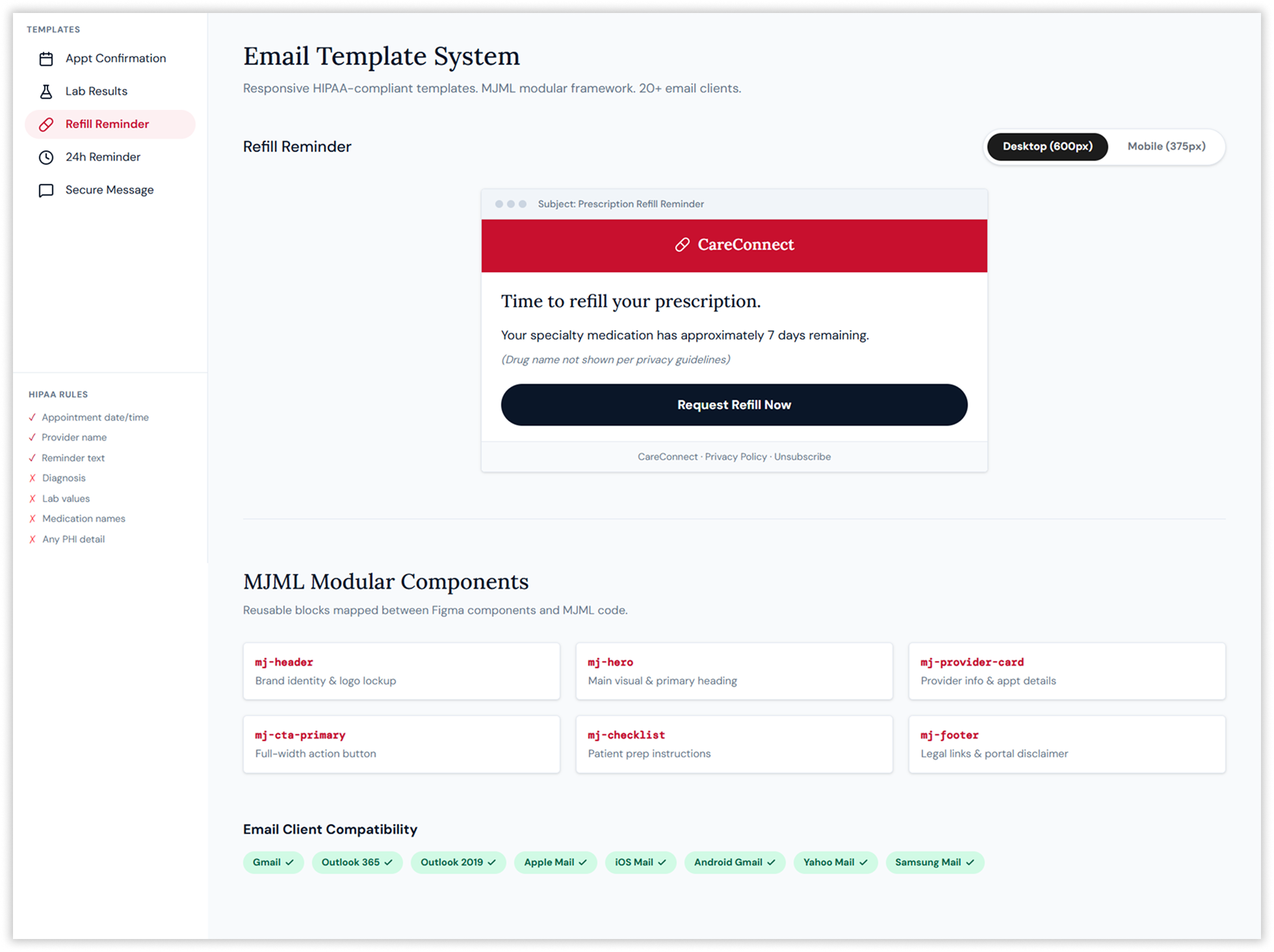
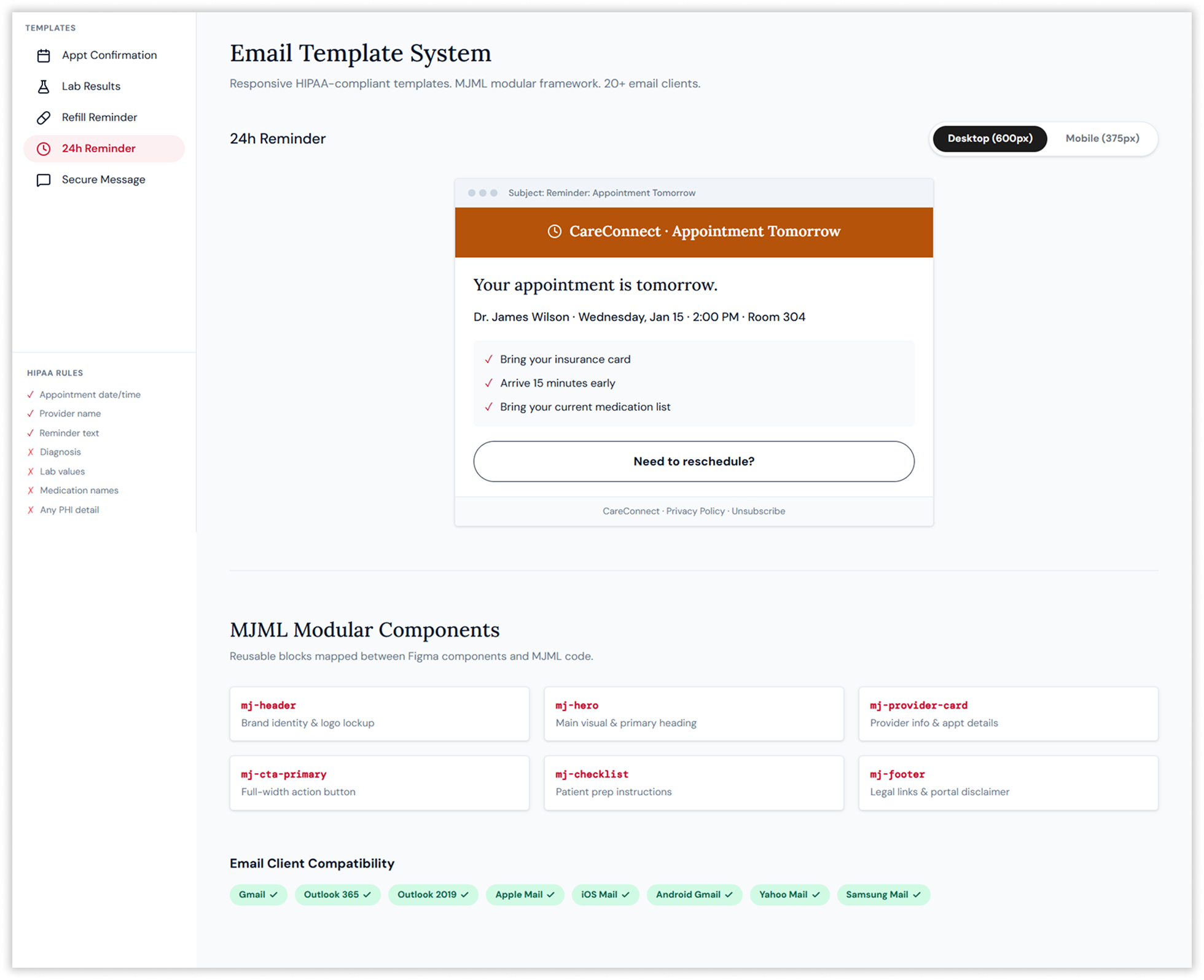
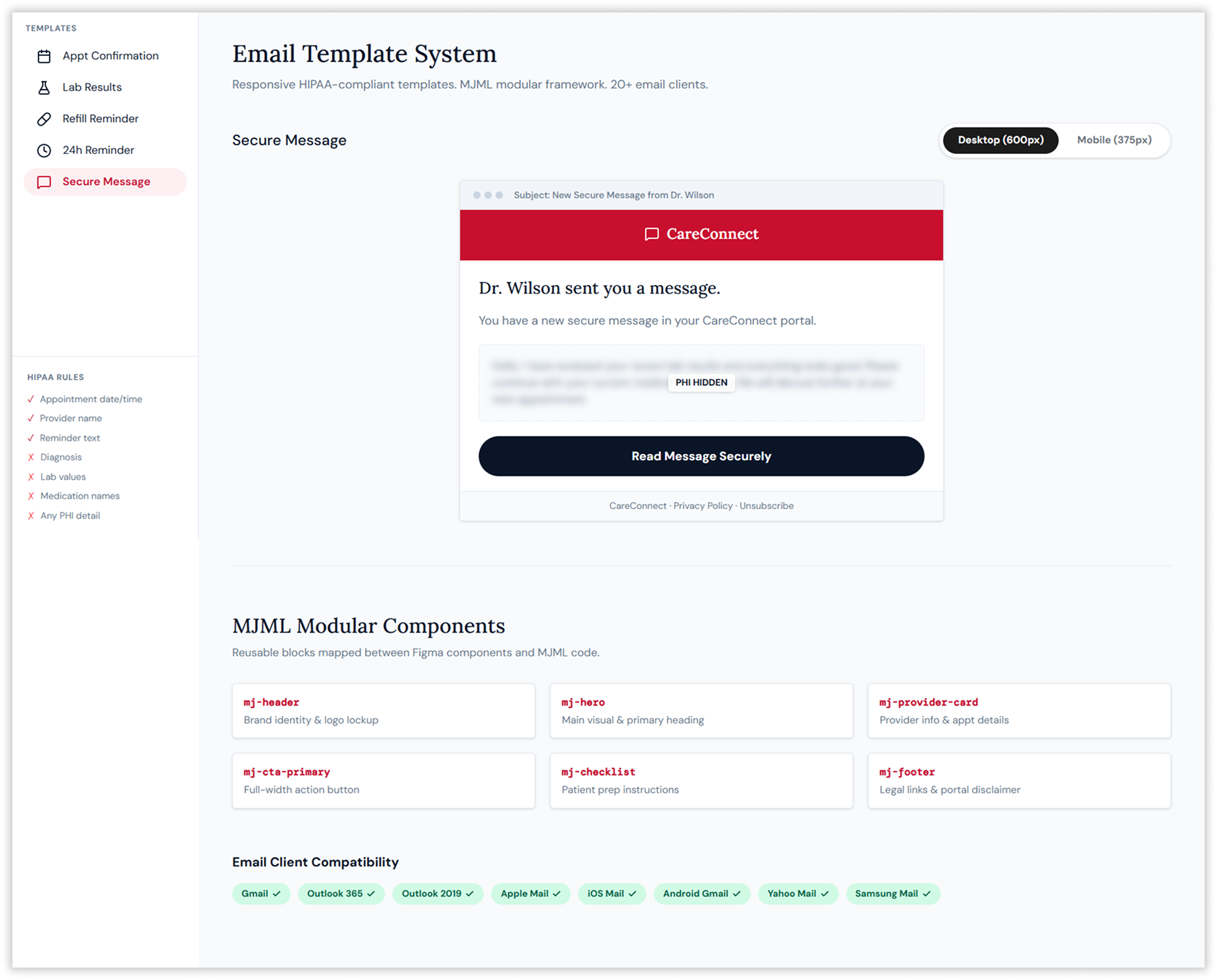
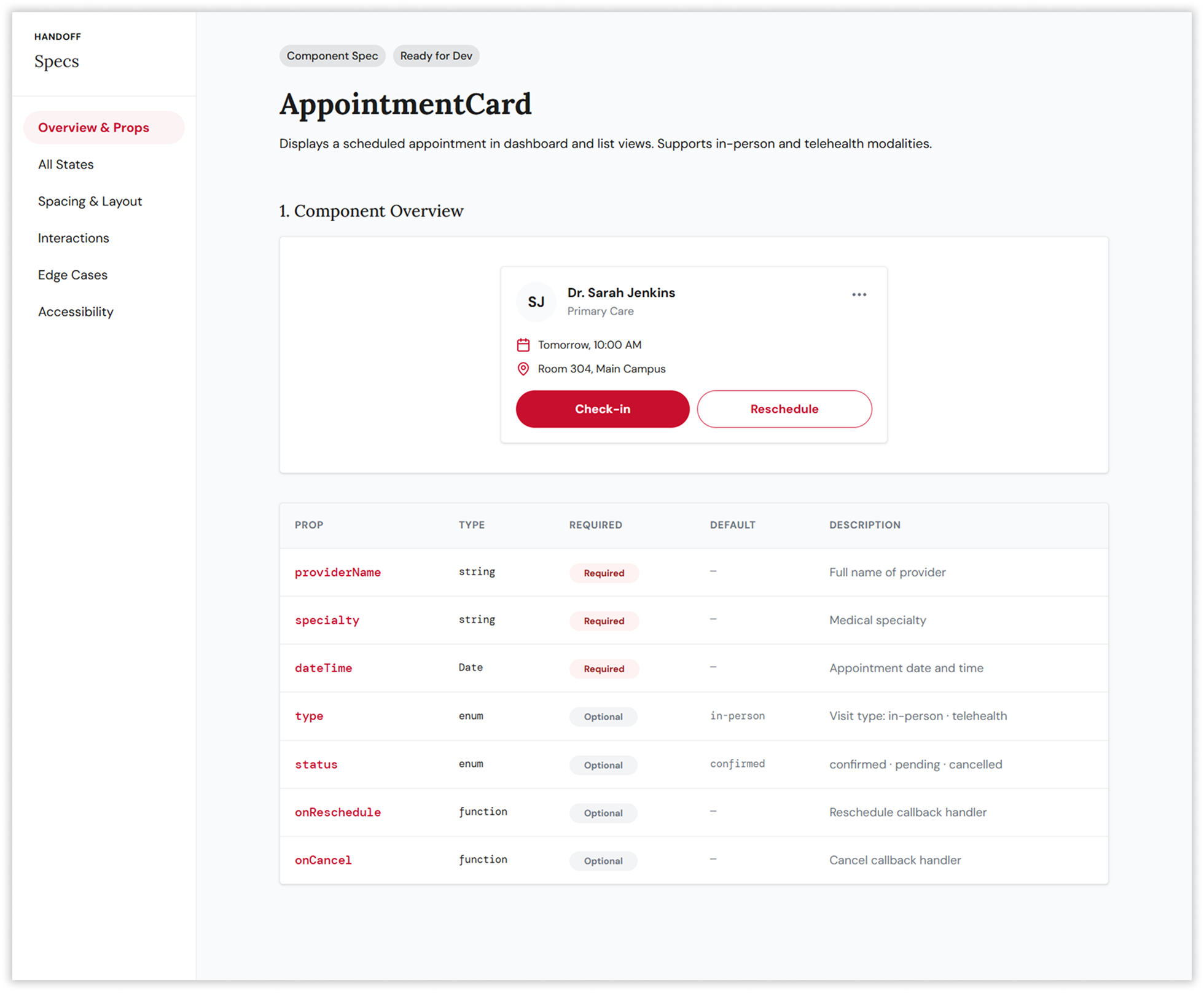
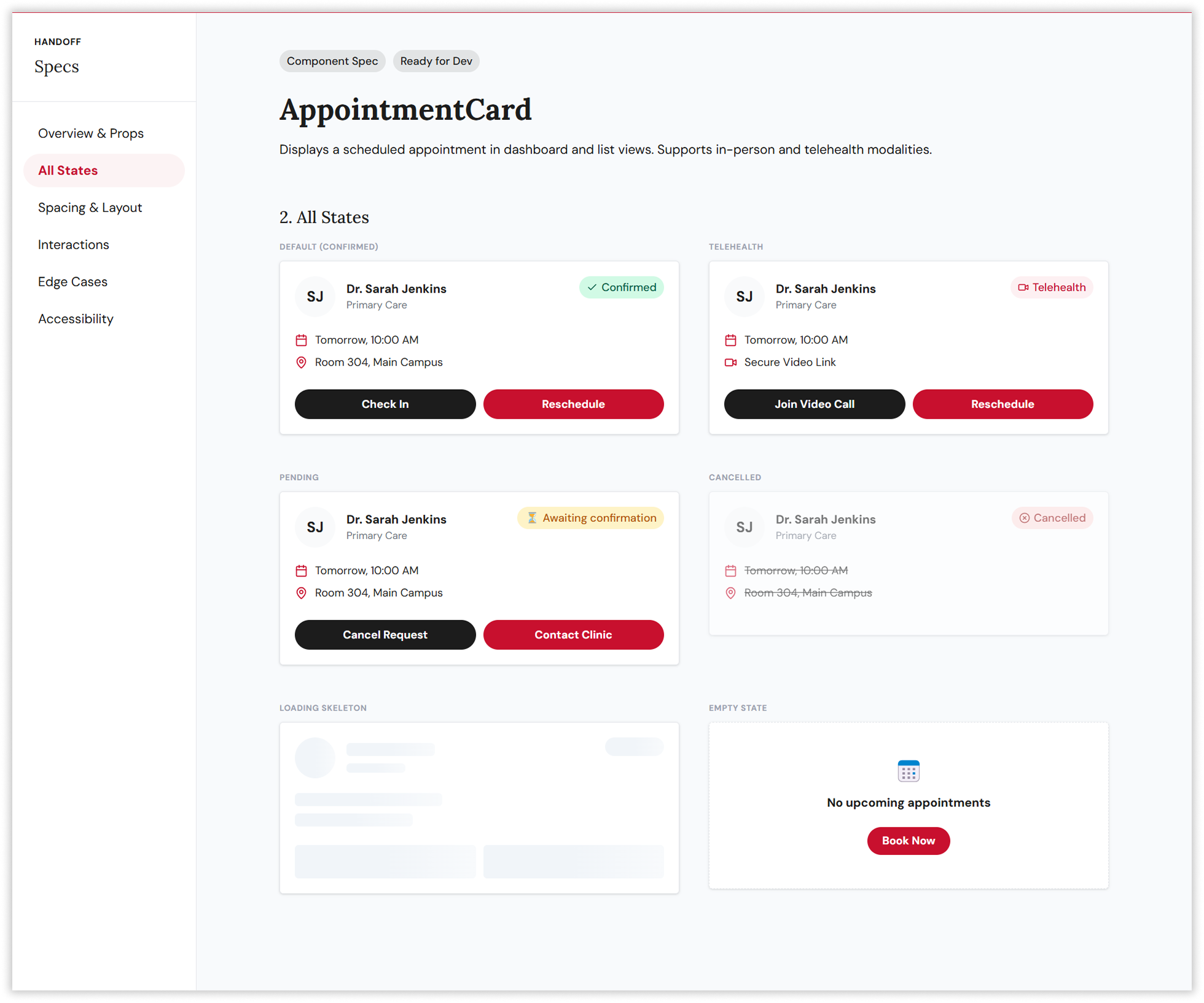
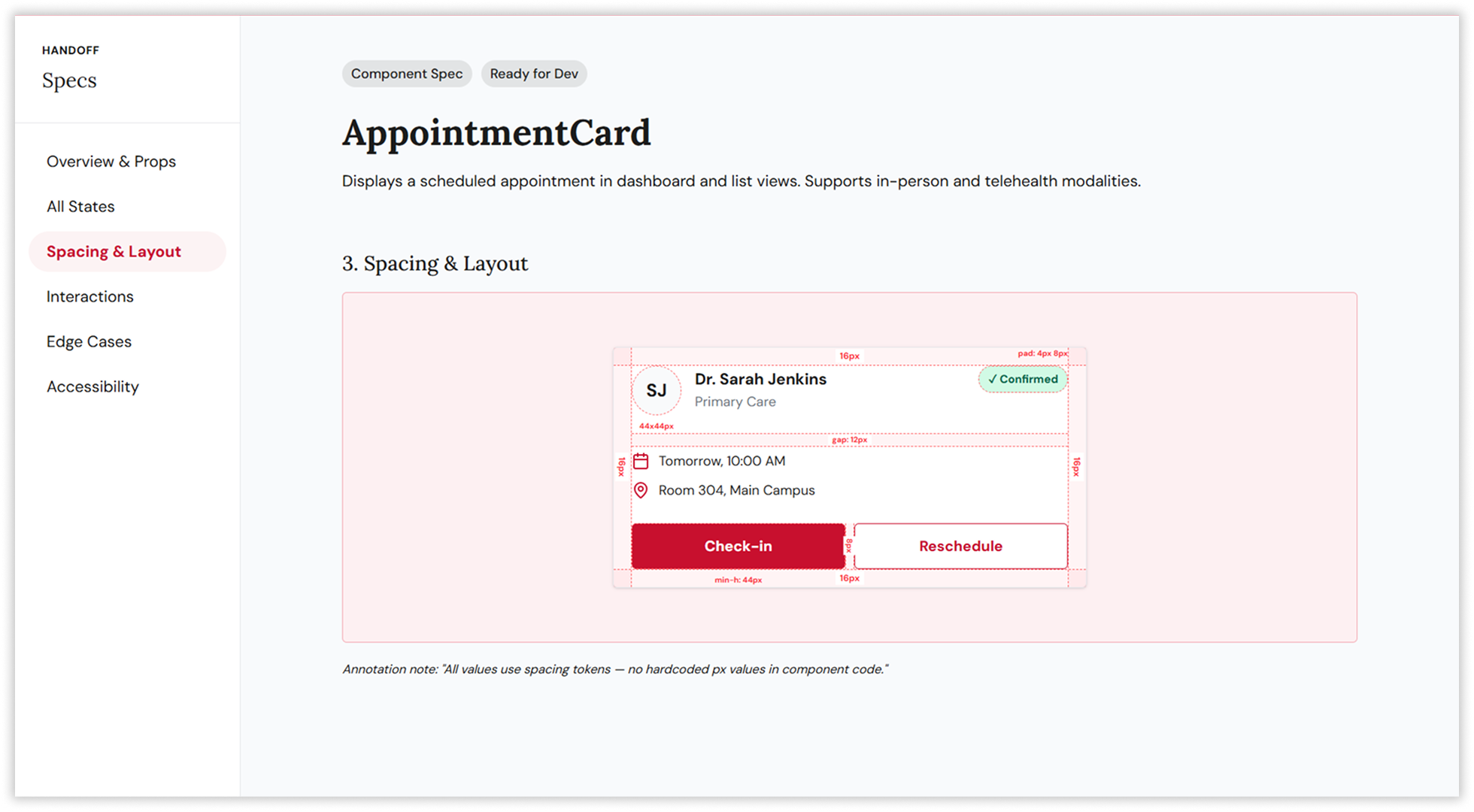
Rather than designing individual screens in isolation, the strategy prioritised building a scalable design system first — 180+ components across six categories, underpinned by a JSON-based design token architecture operating across three tiers: primitive, semantic, and component. This three-tier hierarchy enabled white-label customisation across six global markets (CareConnect US, EuroHealth EU, APACare APAC, and three additional regional variants) from a single codebase, ensuring that a button’s background colour could be updated globally by changing a single token value, not hunting through hundreds of component files.